Heart scarring was detected more than one year after COVID-19 vaccination in some people who suffered myocarditis following receipt of a shot, researchers reported in new studies.
A third of 60 patients with follow-up cardiac imaging done more than 12 months after their myocarditis diagnosis had persistent late gadolinium enhancement (LGE), which is, in the majority of cases, reflective of heart scarring, Australian researchers reported in a preprint of a new study, published on March 22.
Myocarditis is a form of heart inflammation.
The median time from receipt of a vaccine to follow-up imaging was 548 days, with the longest interval being 603 days.
“We found that the incidence of persistent myocardial fibrosis is high, seen in almost a third of patients at >12 months post diagnosis, which could have implications for the management and prognosis of this predominantly young cohort,” the researchers wrote.
“The long-term clinical implications of LGE in this condition are as yet unknown, but LGE has been demonstrated to confer worse prognosis in non-COVID-19 vaccine-associated myocarditis, especially if it persists beyond six months,” they added later, pointing to severalpreviouspapers.
Researchers in one of the previous papers, for instance, found that LGE was a “powerful prognosticator” of adverse outcomes in myocarditis patients.
Before the new testing, nine patients were determined to definitely have myocarditis,and 58 patients were labeled as probably having myocarditis. The findings of persistent LGE resulted in reclassifying 16 of the cases from probable myocarditis to definite myocarditis.
Exclusions included patients who were pregnant or allergic to agents used in gadolinium testing.
Among a subset of 20 patients who underwent imaging shortly after vaccination, 19 had LGE. In follow-up imaging, LGE was no longer visible in 10 of those patients. In five, it was reduced, but in four it was unchanged.
Andrew Taylor, a professor at Monash University’s Central Clinical School, and his co-authors conducted the study by recruiting patients who were diagnosed with myocarditis associated with COVID-19 vaccination between August 2021 and March 2022. The patients were invited to undergo imaging at Alfred Hospital or Royal Children’s Hospital in Melbourne, Australia.
The study population with follow-up imaging included 44 adults and 16 adolescents.
Most of the patients had received a Pfizer-BioNTech shot. A minority had received a Moderna or AstraZeneca vaccination. The companies did not respond to requests for comment.
Limitations of the paper, which was published ahead of peer review, included possible selection bias, since participation in the study was voluntary. Authors listed no conflicts of interest or funding.
Another Paper
In the other recent paper, researchers in Canada reported finding about half of patients referred for imaging due to possible post-vaccination myocarditis had persistent LGE in follow-up imaging.
Overall, 60 patients were included in the retrospective study. Of those, seven reported persistent symptoms.
In a subset of 21 patients for whom follow-up MRIs were available, 10 had persistent LGE, the researchers said. On the other hand, function of the left ventricle, which pumps blood, had normalized in all patients.
The persistent LGE “likely reflects replacement fibrosis,” or heart scarring, Dr. Kate Hanneman, with the University of Toronto’s Department of Medical Imaging, and her co-authors wrote. They cited some of the same papers as the Australian group, including the study that found patients with persistent LGE had a higher risk of adverse outcomes, as well as a paper on what it represents when LGE is found on MRI in patients with myocarditis.
“However, the significance of LGE is uncertain in patients post-myocarditis with recovered normal left ventricular systolic function,” the researchers said. They called for additional studies to evaluate patients with persistent LGE and a recovered left ventricle.
The study included adult patients who were referred to a hospital network with suspected myocarditis and had new cardiac symptoms such as chest pain within 14 days of COVID-19 vaccination. The patients all received either the Pfizer or Moderna shot.
Limitations of the study, which was published by the Journal of Cardiovascular Magnetic Resonance, included a lack of biopsy-confirmed myocarditis.
The authors declared no funding and listed only one competing interest, that an author is an associate editor of the journal.
The corresponding authors for the two papers did not respond to requests for comment.
“My concern from reading these two studies is that myocardial damage and scarring is present in a significant number of COVID vaccine injured individuals at up to 18 months after vaccination. This suggests potential for permanent heart damage from the vaccines,” Dr. Danice Hertz, the research lead for the U.S. group React19, told The Epoch Times in an email. “The long-term implications are not yet known but need to be studied carefully.”
Earlier Findings
The new papers add to earlier studies, which found that LGE persists for months in some people following a COVID-19 shot.
Researchers in Washington state reported in 2022 that LGE persisted in children for up to eight months after vaccination. Later that year, the U.S. Centers for Disease Control and Prevention (CDC) said that more than half of 151 patients with follow-up imaging had residual LGE, which was described as “suggestive of myocardial scarring.”
The CDC has longer-term data on the patients, the agency confirmed to The Epoch Times in January, but has not yet published another paper describing that data. The CDC, which failed to warn the public about the risk of post-vaccination myocarditis, declined to comment on the new Australian and Canadian papers.
Hong Kong researchers in 2023 reported finding that about half of 40 patients with follow-up MRIs months after vaccination had LGE.
Symptoms have also persisted in some patients with post-vaccination myocarditis.
The CDC, describing preliminary updated results from its longer-term study, said in early 2023 that there were patients still suffering from symptoms more than one year after a shot. Researchers in Australia in late 2023 said that symptoms persisted at least six months after a shot in a majority of patients they followed. And some patients also told The Epoch Times they have lingering health issues years after vaccination.
In mid-February, the leader of Moldova’s breakaway region of Transnistria, Vadim Krasnoselsky, summoned deputies “of all levels of the Pridnestrovian Moldavian Republic”. The purpose of their meeting, he announced, would be to discuss “pressure from the Republic of Moldova that is violating the rights and worsening the socioeconomic situation of Transnistrians”.
The meeting was set for February 28, the day before Vladimir Putin’s “state of the union” address. This was taken by some – including the influential Washington-based thinktank the Institute for the Study of War – to signal an intention to announce that Transnistria would formally declare its intention to join Russia.
The Transnistrian congress met as planned. But its resolution, while full of praise about Transnistria and complaints about Moldova, fell well short of expectations. In the end, the assembled deputies merely appealed to Russia – as well as the Interparliamentary Assembly of States Parties of the Commonwealth of Independent States, the UN, the EU, the Organization of Security and Co-operation in Europe, and the Red Cross – to protect Transnistria and prevent an escalation of tensions with Moldova.
Transnistria declared independence from the Moldovan Soviet Socialist Republic in 1990, as the dissolution of the Soviet Union was gathering pace. A brief violent conflict ended with a Russian-mediated ceasefire in 1992. This ceasefire mandated negotiations on the reintegration of Transnistria into Moldova, which included, among others, Russia and Ukraine. Efforts to agree on a deal proved futile over the following three decades and have completely stalled since Russia’s full-scale invasion of Ukraine in February 2022. Thus, the Transnistrian region of Moldova has remained in a limbo state for more than 30 years now. Its separate identity is not even recognised by Russia and it remains formally part of Moldova.
In the event, the Russian president failed to mention Transnistria even once in his state of the union address the day after deputies had gathered in Transnistria. With the initial “excitement” of a potential crisis around Moldova gone, the predominant view among regional and international analysts was that this was a storm in a tea cup rather than a full-blown crisis.
This is also the view of Moldova’s foreign minister, Mihail Popșoi. In an interview with Politico at the beginning of March, a month after taking office, Popșoi said that “the probability that the Russians would be able to advance and reach our territory is much lower now than it was two years ago”.
Russian ambitions
But this is, at best, only half of the more complex geopolitical context in which Moldova finds itself. Wedged between Ukraine and Romania, a member of Nato, Moldova’s future prospects are heavily intertwined with the outcome of the war against Ukraine. At present there appears to be little chance of Russia expanding its land bridge to Crimea all along the Black Sea coast to the Ukrainian border with Moldova. But that’s not to say that the Kremlin has completely given up on this ambition.
Just days after the deputies’ meeting in Transnistria, the Russian foreign minister, Sergey Lavrov, complained about Moldovan violations of Transnistria’s rights. He alleged Moldovan discrimination against the Russian language as well as economic pressure on the Russian enclave. This eerily echoes Russian justifications for the invasion of Ukraine both in 2014 and 2022.
Transnistria is not the only card Russia is playing. Four days after Lavrov’s comments, Putin met the leader of the Gagauzian region in Moldova, Yevgenia Gutsul, at the so-called World Youth Festival, which was held near the Russian Black Sea resort of Sochi at the beginning of March.
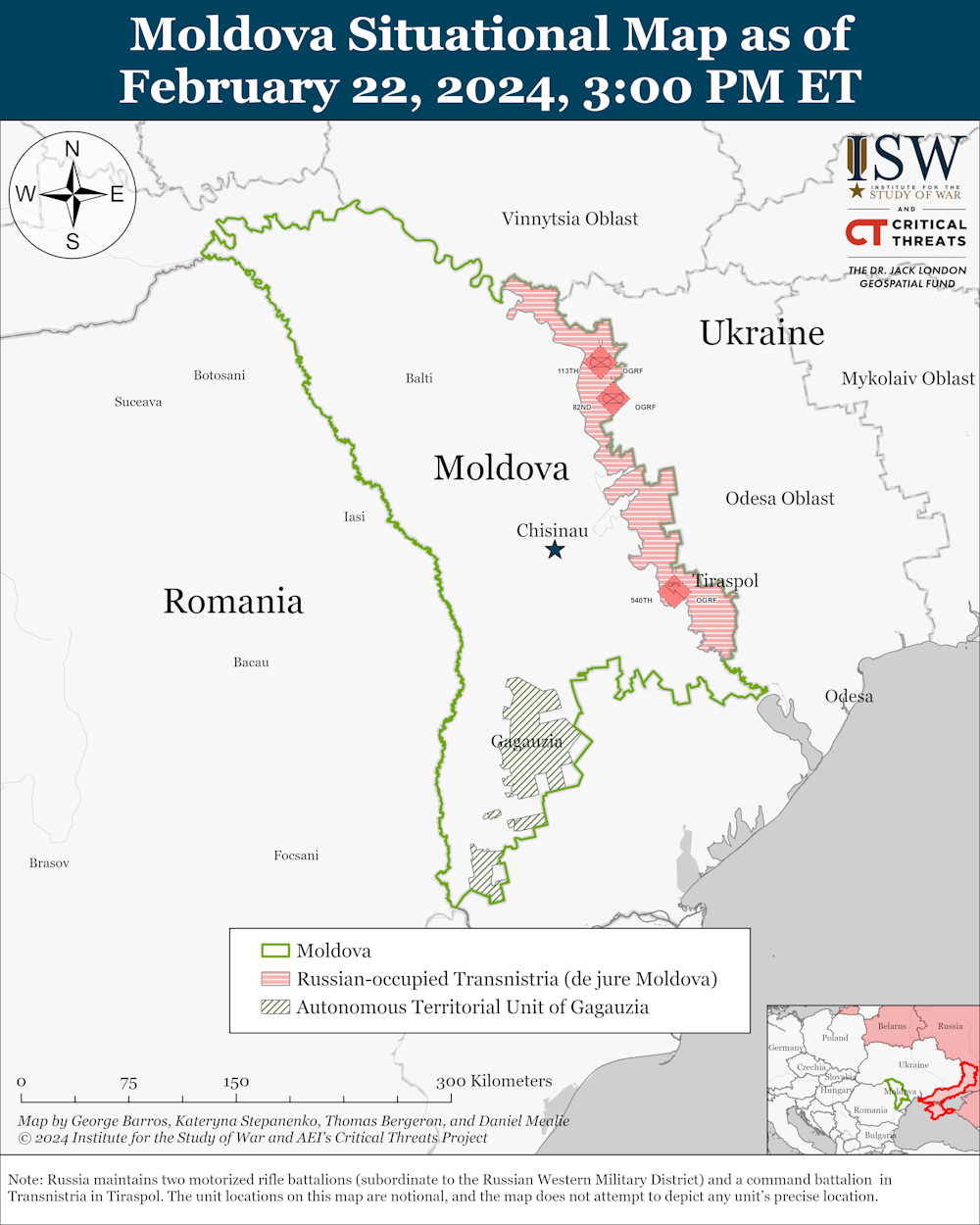
Map of Moldova showing the breakaway regions of Transnistria and Gaugazia.Institute for the Study of War
Gutsul – and other powerful Russian allies including the fugitive Moldovan oligarch Ilan Shor, who was convicted of fraud in the “theft of the century” of US$1 billion (£792 million) from three Moldovan banks a decade ago – have been fomenting protests against the Moldovan government since September 2022. These protests reflect many ordinary Molovans’ existential fears over a cost-of-living crisis that has engulfed one of Europe’s poorest countries since the COVID pandemic and has worsened since the Russian aggression against Ukraine.
Moldova’s European aspirations
At the same time, the Moldovan president, Maia Sandu, has proposed a referendum on joining the European Union. Sandu, who faces a reelection campaign later this year, hope that this will boost her popularity among Moldova’s generally – but not unequivocally – pro-European electorate.
Wanting to capitalise on popular discontent with economic conditions in Moldova, Russia has been supporting Shor’s protests and linking the unrest to Sandu’s pro-European foreign policy. Relying on allies in both Gagauzia and Transnistria, Moscow’s aim is primarily the destabilisation of the country ahead of presidential elections at the end of 2024 and parliamentary elections in the spring of 2025.
In this context, even non-events such as the resolution passed by the Transnistrian deputies at the end of February are useful to Moscow. They increase uncertainty not only in Moldova but also among the country’s western allies. And this feeds into a broader narrative in which a status quo that has been stable for decades is suddenly questioned – with potentially unpredictable consequences.
There is no evidence that the Kremlin has any concrete plans, let alone any capabilities, for military action against Moldova. Nor does it need to, as long as it has local allies to do its bidding against the country’s president and her government. This does not give Moscow a lot of leverage in its war against Ukraine but it is helpful in the broader efforts to weaken support for, and from, the European Union.
The more Russia can peddle a narrative that connects European integration with economic decline and constraints on language and cultural rights, the more division it can sow – and not just in Moldova, but potentially also in other EU candidate countries from the western Balkans to the south Caucasus.
Stefan Wolff is a past recipient of grant funding from the Natural Environment Research Council of the UK, the United States Institute of Peace, the Economic and Social Research Council of the UK, the British Academy, the NATO Science for Peace Programme, the EU Framework Programmes 6 and 7 and Horizon 2020, as well as the EU's Jean Monnet Programme. He is a Trustee and Honorary Treasurer of the Political Studies Association of the UK and a Senior Research Fellow at the Foreign Policy Centre in London.
Blueprint for mandating indoor air quality for public buildings in form of standards
Credit: QUT International experts set out standards for monitoring three key indoor pollutants Adequate ventilation for number of occupants and activities…
International experts set out standards for monitoring three key indoor pollutants
Adequate ventilation for number of occupants and activities must be taken into account
Carbon dioxide and PM2.5 particles and carbon monoxide are three pollutants requiring monitoring to assess healthy
The experts addressed setting standards for three key indoor pollutants – carbon dioxide (CO2), carbon monoxide (CO), PM2.5 which are particles so small they can lodge deep in the lungs and enter the bloodstream – and ventilation rate.
Distinguished Professor Morawska, from the QUT School of Earth and Atmospheric Sciences, internationally known, among others, for leading the appeal to the WHO to recognise the airborne transmission spread of the Covid-19 virus early in the pandemic, has continued to raise the importance of adequate indoor air quality for public spaces.
“Most countries do not have any legislated indoor air quality (IAQ) performance standards for public spaces that address concentration levels of IA pollutants,” Professor Morawska said.
“To have practical value, IAQ standards must be implementable by designing new buildings that are built, operated and maintained to standard or retrofitted to meet the standards.
“While there is a cost in the short term, the social and economic benefits to public health, wellbeing and productivity will likely far outweigh the investment in cost in achieving clean indoor air.”
Professor Morawska said CO2 sensors were readily available, inexpensive and robust and should be used as a proxy to measure pathogens and CO2 during human occupancy in a public space.
“CO2 can serve as a proxy for occupant-emitted contaminants and pathogens and to effectively assess ventilation quality,” she said.
“We propose a CO2 concentration level of 800ppm with the proviso that outdoor concentration is used as a baseline and recognition of the fact that outdoor concentrations are increasing due to emissions to the atmosphere that outweigh removal.
“Another key indicator of air quality we addressed is the amount of PM2.5 and we propose the WHO air quality guidelines as a basis for indoor air quality standards but with a 1-hour averaging time, as the 24 hours of the WHO AQG is much longer than people usually spend in public places.”
Professor Morawska said mechanical ventilation systems should remove and dilute human-emitted and other indoor-generated pollutants at a higher rate than their production so that they would not accumulate in indoor air.
“The technologies for measuring ventilation already exist in most modern mechanically ventilated buildings but monitoring ventilation rates in terms of clean air delivered to the space requires us to consider the number of people and their activities in the space to ensure adequate IAQ.
“A practical ventilation standard could be air from outside (assumed to be clean), or clean recirculated air to the entire occupied zone and with airflow not directed from one person to another.
“Additional measures in support of ventilation, such as air cleaning and disinfection, could greatly reduce the need to increase the outdoor air supply, which carries a heavy energy demand.
“Filtering recirculated air is an effective way to reduce concentration of, and thus our exposure to, airborne particulate matter, allergens and pathogens.”
Mandating indoor air quality standards in public buildings was published in Science.
The expert contributors were Professor Morawska, Professor Belinda Bennett, and Professor Amanda Kennedy, QUT, Australia; Associate Professor Joseph Allen, Harvard University, USA; Professor William Bahnfleth, The Pennsylvania State University, USA; Professor Philomena M. Bluyssen and Professor Atze Boerstra, Delft University of Technology, The Netherlands; Professor Giorgio Buonanno, University of Cassino and Southern Lazio, Cassino, Italy; Professor Junji Cao, Chinese Academy of Science, China; Professor Stephanie J. Dancer, Edinburgh Napier University, UK; Professor Andres Floto and Dr Charles Haworth, University of Cambridge, UK; Francesco Franchimon, Franchimon ICM, The Netherlands; Professor Trish Greenhalgh, University of Oxford, UK; Jaap Hogeling, International Standards at ISSO, The Netherlands; Associate Professor Christina Isaxon and Associate Professor Aneta Wierzbicka, Lund University, Sweden; Professor Jose L. Jimenez and Professor Shelly L. Miller, University of Colorado, USA; Professor Prashant Kumar, University of Surrey, UK; Professor Jarek Kurnitski, Tallinn University of Technology, Estonia; Professor Yuguo Li, University of Hong Kong, China; Associate Professor Marcel Loomans, Eindhoven University of Technology, The Netherlands; Professor Guy Marks, University of New South Wales; Professor Linsey C. Marr,Virginia Tech, USA, Professor Livio Mazzarella, Politecnico di Milano, Italy; Professor Arsen Krikor Melikov and Professor Pawel Wargocki, Technical University of Denmark, Denmark; Professor Donald K. Milton, University of Maryland; Professor Jason Monty, University of Melbourne, Australia; Associate Professor Peter V. Nielsen, Aalborg University, Denmark; Professor Catherine Noakes, University of Leeds, UK; Professor Jordan Peccia, Yale University, USA; Professor Kimberly A. Prather, University of California, USA; Professor Xavier Querol, Institute of Environmental Assessment and Water Research, Spain; Professor Tunga Salthammer, Fraunhofer WKI, Germany; ProfessorChandra Sekharand Associate Professor Kwok Wai Tam, National University of Singapore, Singapore; Associate Professor Olli Seppänen, Aalto University Finland; Professor Shin-ichi Tanabe, Waseda University, Japan; Associate ProfessorJulian W. Tang, University of Leicester, UK; Associate Professor Raymond Tellier, McGill University, Canada; Professor Maosheng Yao,, Peking University, China.
RNA-based immunizing agents have enriched the repertoire of technologies used for vaccine development. An analysis of the active clinical trials in early…
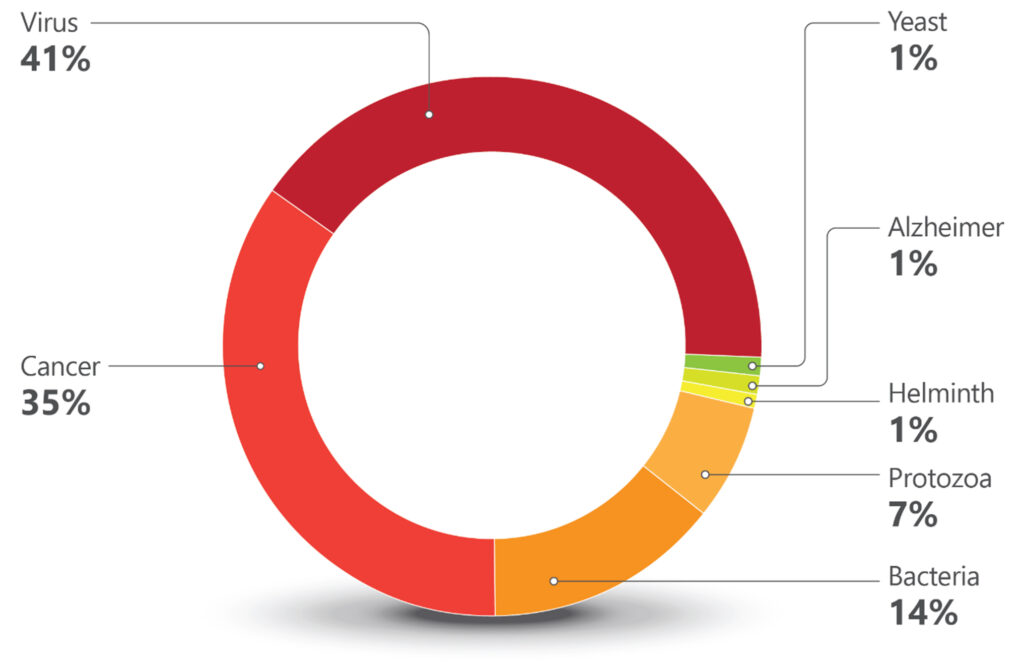
RNA-based immunizing agents have enriched the repertoire of technologies used for vaccine development. An analysis of the active clinical trials in early Phase I and Phase I during the year of 2023 illustrates this point. A total of 161 active vaccine trials were registered at clinicaltrials.gov. Information from these trials was used to plot (Chart 1) and (Chart 2) SARS-CoV-2/COVID-19 trials were excluded to give more evidence to other disease targets.
Chart 1. Targets for Vaccines in Early Stages of Clinical Development. Early Phase I and Phase I clinical trials were grouped according to the diseases (cancer or Alzheimer) or type of infectious agents (viruses, bacteria, protozoa, helminth, and yeast). One-hundred-sixty-one trials were identified using vaccine as keyword and filters for active trials and therapeutic intervention during the period of 01/01/2023 to 1/7/2024. COVID 19/SARS-CoV-2 related trials were excluded. [clinicaltrials.gov]The highest number of trials were against viral infections (67 trials). Most have influenza, Herpes zoster, RSV (Respiratory Syncytial virus), and HIV as targets. The commercially available flu vaccines do need improvement and RNA technologies provide hope for better products. Different companies are exploring this space, including Moderna, Sanofi, Pfizer, Arcturus, Seqirus, and GSK.
The commercial success of Shingrix®, the GSK vaccine against Herpes zoster, has led to five companies in China to follow suit with their own products. Moderna is also pursuing the shingles market with an mRNA-based candidate, while Immorna (China) is testing a self-replicating RNA vaccine. Another competitive market is vaccines for respiratory tract infections. RSV is the leading causative agent for lower track respiratory diseases, causing 3.4 million hospitalizations and 950,00–150,000 deaths every year.
Until recently, no vaccines against the virus were commercially available, but two were approved by the FDA in 2023. Arexvy® from GSK, was approved for older adults, and Abrysvo® from Pfizer, for adults and pregnant women (to protect infants from birth to six months). Four other companies are developing vaccines against RSV.
Blue Lake Biotechnology (U.S.) and Codagenix (U.S.) are testing pediatric vaccines. The former is working on an intranasal recombinant parainfluenza virus type 5 for infants and children, and the latter, also developing an intranasal pediatric vaccine, but based on a live-attenuated engineered virus. Sanofi has two trials, one for infants (intranasal) based on live attenuated virus and one for adults (intramuscular) against both RSV and hMPV (human metapneumovirus).
Targeting both these viruses in one jab is also in Moderna’s and AstraZeneca’s pipeline. While Moderna is developing an mRNA-based formulation for infants, AstraZeneca, through the acquisition of Icosavax, has a VLP (Virus-Like Particle) platform technology with a lead program targeting both viruses[1].
Decades of difficulties in the development of vaccines against HIV resulted in many companies dropping their research programs targeting the virus. Of the eight ongoing trials, seven are sponsored by research institutions and only one is sponsored by a company, Vir Biotechnology.
Second largest target
The second largest target in number of trials is cancer (56 trials). The vast majority involve the development of immunotherapies and a recurrent approach are therapeutic vaccines using dendritic cells loaded with personalized neoantigens. Ten out of the 56 cancer trials are based on RNA technologies. Nature’s publication from June 2023[2], showing promising results of a personalized neoantigen mRNA immunotherapy for pancreatic cancer, indicated the feasibility of this complex approach.
The number of companies as sponsors of early-stage trials for vaccines for cancer is smaller than that for viral infections (many cancer trials are sponsored by research/academic institutions). Nevertheless, a good proportion of the company-sponsored trials are for cancers associated with viruses, such as is the case for the HPV vaccines. The vast majority of cervical cancers is associated with the presence of the HPV virus and immunization programs almost eliminated cervical cancer in women born in England since 1995[3].
It is reasonable to hope that the vaccines being developed for EBV (Epstein–Barr virus) or CMV (Cytomegalovirus) associated cancers (hematological malignancies and glioblastomas, respectively) can be successful as well. Immunomic Therapeutics has a DNA formulation based on its UNITE® proprietary technology that explores the CMV-GBM association.
The twelve trials in the protozoa group (Chart 1) are all against just one protozoan, Plasmodium, the causative agent of malaria. Six are sponsored by the University of Oxford. R21, the vaccine developed by Oxford University and the Serum Institute of India, is based on a recombinant protein. It is the second vaccine recommended by the WHO for malaria, a fusion recombinant product which is part circumsporozoite protein of Plasmodium falciparum and part Hepatitis B surface protein antigen.
Recombinant construct
Expressed in yeast, this recombinant construct is more immunogenic and cheaper to manufacture than Mosquirix® (the first malaria vaccine recommended by WHO, developed by GSK)[4]. It is worthy to note that all formulations in University of Oxford’s trials employ the Matrix-MTM adjuvant, which was developed by Novavax and is made with compounds from the bark of the Chilean tree Quillaja saponaria[5].
Twenty trials are registered against bacterial infections: tetanus, diphtheria, Shigellosis, pneumococcal, streptococcal, and meningococcal infections, tuberculosis, and Lyme Disease are the targets. Old unmet medical needs, such as Lyme disease and tuberculosis, are being addressed (also) by mRNA technologies. The Austrian company Eveliqure has a new approach for attenuating genetically engineered bacteria and is testing its oral ShigETEC against Shigellosis. In Australia, GPN Vaccines innovated on inactivation of whole organisms and is using its technology against pneumococcal infections.
Chart 2. Technologies Used for Vaccine Development. [Golgher and Rodrigues]Lastly are the trials that comprise a low percentage of the pipeline, which is unfortunate since they address unmet medical needs of millions. There is just one trial against helminths, against schistosomiasis, a disease that affects 240 million people. Sponsored by the International Vaccine Institute, it has Seattle-based PAI Life Sciences as a collaborator.
Two trials are against Alzheimer disease, both sponsored by research institutions. One is a DNA based vaccine that aims to elicit antibodies against amyloid-β.The other, interestingly, is testing if the BCG vaccine (Bacillus Calmette–Guérin) has an effect on reducing biomarkers for the disease. BCG vaccines are based on attenuated forms of the bacterium Mycobacterium bovis.
The only trial against a fungal infection targets yeast. The goal is to generate protection for women who experience recurrent vulvovaginal candidiasis, and the trial is sponsored by the Swiss company LimmaTech Biologics, in collaboration with GSK. There are no available vaccines against fungal infections, which are responsible for an annual global death rate of approximately 1.5 million[6].
More input needed from South America
Interesting points could be drawn from the analysis of the ongoing early Phase I and Phase I clinical trials on vaccines. There were more European biotechnology companies (11) (Austria, Denmark, France, Germany, Switzerland, Sweden) plus one in the U.K., than there were American companies (10).
By adding the Australian and Asian companies in early stages clinical trials, there were 30 biotechs dedicated to the development of interesting immunizing agents. By mix and matching old approaches (inactivated or attenuated) with more modern ones (recombinant proteins, fusion constructs, VLPs, RNA, DNA), using systems biology, genetic engineering, AI), innovation in vaccines is flourishing. See Figure 1.
Figure 1. Novel, and not so novel, technologies incrementing the vaccine pipeline. [Golgher and Rodrigues]Some of the diseases studied by the companies developing these early-stage clinical trials are predominantly health problems of low- and middle-income countries. It is disappointing to note the absence of companies from South America among the sponsors or collaborators in these trials. According to IQVIA, the global vaccine market (excluding COVID-19) reached $39 billion in 2022, with a growth rate of seven percent CAGR between 2017–2022[7]. The market is mostly driven by innovative vaccines and is bound to grow. South American countries must work to have a better share of it.
Brazil has an admirable vaccination program and internationally recognized governmental vaccine factories (Butantan and Biomanguinhos), but a poor track record on innovation in this area[8]. It is senseless to invest so much in the training of excellent immunologists, vaccinologists, and infectious disease experts and not translate this into novel products. A lot more can be done.
If it depends on the initiative, CTVacinas (soon to be CN Vaccines, CN for National Center), coordinated by the researcher Ricardo Gazzinelli, DSc, DVM, Oswaldo Cruz Foundation and Universidade Federal de Minas Gerais (UFMG), it will be done.
For those who know Gazzinelli, it is easy to bet that the enterprise under his leadership, which includes the collaboration of several other researchers from UFMG, will thrive. When it comes to partnerships, CTVacinas is open and agnostic; what matters is that meaningful projects move forward, and partners can come from private, public, international or national institutions. An important part of their mission is to be an institute good at translating academic research into novel immunizing formulations. The aim is to generate more businesses, products, and startups.
CTVacinas has a history: part of its revenues come from royalties from a vaccine for dogs against visceral leishmaniasis, developed by Gazzinelli and his business partner, Ana Paula Fernandes.
Figure 2. Ricardo Gazzinelli, pictured on the right and the CTVacinas team on the left. CTVacinas is located at UFMG’s technology park, it is a leading organization in developing vaccine projects that can become innovative products and businesses. The initiative has secured funds for expansion. [CTVacinas]In CTVacinas pipeline is SpiN-Tec, a vaccine against SARS-CoV-2, now in Phase II trials. It is the first 100% Brazilian vaccine. SpiN-Tec is a made of a recombinant fusion product of the S and N proteins of the virus, and the hope is that it will confer protection irrespective of the strain.
Helton Santiago, MD, PhD, a professor at UFMG who works with Gazzinelli, is responsible for SpiN-Tec’s clinical program, among others. He is an enthusiastic member of the CTVacinas vaccine team and is optimistic about the future of Brazil in the vaccine field. According to Santiago, the COVID-19 pandemic stimulated the national players to move at a faster pace toward innovation.
If some needed a pandemic to shake them out of a sluggish mode, others have started out going as fast as possible. It is the case, for example, of Luana Raposo, Bruna Porchia, and Mariana Diniz, founders of ImunoTera, a spinoff from the University of São Paulo (Figure 3). With proprietary technology developed during their PhDs, they have succeeded in securing funds for their company’s first steps.
Figure 3. Founders of ImunoTera, Luana Raposo (left) and Bruna Porchia (right) at the Albert Einstein Hospital. ImunoTera was one of the startups selected for the hospital’s biotechnology program. [Tauan Sousa]ImunoTera is dedicated to developing immunotherapies against infectious diseases and cancer and has been selected for competitive preincubation and incubation programs in the country. The founders have chosen wisely and, with the support of the best programs and partners to develop their pipeline, are advancing. Their first product has been tested in patients with HPV-induced high grade cervical neoplasia, with promising results. ImunoTera may be the one to develop the next 100% Brazilian vaccine.
Denise Golgher, PhD (d.golgher@gmail.com) is a life sciences consultant based in São Paulo, Brazil. Rob Rodrigues, LLM, Stanford Law School, is a partner at Licks Attorneys. Many thanks to our interviewees, Luana Raposo from Imunotera, Walderez Dutra from UFMG, Ricardo Gazzinelli and Helton Santiago from CT vacinas, Eduardo Levi from DASA, Jorge Kalil from USP and Constantino Lopez from Instituto Mexicano del Seguro Social.
We use cookies on our website to give you the most relevant experience by remembering your preferences and repeat visits. By clicking “Accept”, you consent to the use of ALL the cookies.
This website uses cookies to improve your experience while you navigate through the website. Out of these, the cookies that are categorized as necessary are stored on your browser as they are essential for the working of basic functionalities of the website. We also use third-party cookies that help us analyze and understand how you use this website. These cookies will be stored in your browser only with your consent. You also have the option to opt-out of these cookies. But opting out of some of these cookies may affect your browsing experience.
Necessary cookies are absolutely essential for the website to function properly. These cookies ensure basic functionalities and security features of the website, anonymously.
Cookie
Duration
Description
cookielawinfo-checbox-analytics
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Analytics".
cookielawinfo-checbox-functional
11 months
The cookie is set by GDPR cookie consent to record the user consent for the cookies in the category "Functional".
cookielawinfo-checbox-others
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Other.
cookielawinfo-checkbox-necessary
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookies is used to store the user consent for the cookies in the category "Necessary".
cookielawinfo-checkbox-performance
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Performance".
viewed_cookie_policy
11 months
The cookie is set by the GDPR Cookie Consent plugin and is used to store whether or not user has consented to the use of cookies. It does not store any personal data.
Functional cookies help to perform certain functionalities like sharing the content of the website on social media platforms, collect feedbacks, and other third-party features.
Performance cookies are used to understand and analyze the key performance indexes of the website which helps in delivering a better user experience for the visitors.
Analytical cookies are used to understand how visitors interact with the website. These cookies help provide information on metrics the number of visitors, bounce rate, traffic source, etc.
Advertisement cookies are used to provide visitors with relevant ads and marketing campaigns. These cookies track visitors across websites and collect information to provide customized ads.















































{kind=link}
{kind=link}