Blueprint for mandating indoor air quality for public buildings in form of standards
Credit: QUT International experts set out standards for monitoring three key indoor pollutants Adequate ventilation for number of occupants and activities…
International experts set out standards for monitoring three key indoor pollutants
Adequate ventilation for number of occupants and activities must be taken into account
Carbon dioxide and PM2.5 particles and carbon monoxide are three pollutants requiring monitoring to assess healthy
The experts addressed setting standards for three key indoor pollutants – carbon dioxide (CO2), carbon monoxide (CO), PM2.5 which are particles so small they can lodge deep in the lungs and enter the bloodstream – and ventilation rate.
Distinguished Professor Morawska, from the QUT School of Earth and Atmospheric Sciences, internationally known, among others, for leading the appeal to the WHO to recognise the airborne transmission spread of the Covid-19 virus early in the pandemic, has continued to raise the importance of adequate indoor air quality for public spaces.
“Most countries do not have any legislated indoor air quality (IAQ) performance standards for public spaces that address concentration levels of IA pollutants,” Professor Morawska said.
“To have practical value, IAQ standards must be implementable by designing new buildings that are built, operated and maintained to standard or retrofitted to meet the standards.
“While there is a cost in the short term, the social and economic benefits to public health, wellbeing and productivity will likely far outweigh the investment in cost in achieving clean indoor air.”
Professor Morawska said CO2 sensors were readily available, inexpensive and robust and should be used as a proxy to measure pathogens and CO2 during human occupancy in a public space.
“CO2 can serve as a proxy for occupant-emitted contaminants and pathogens and to effectively assess ventilation quality,” she said.
“We propose a CO2 concentration level of 800ppm with the proviso that outdoor concentration is used as a baseline and recognition of the fact that outdoor concentrations are increasing due to emissions to the atmosphere that outweigh removal.
“Another key indicator of air quality we addressed is the amount of PM2.5 and we propose the WHO air quality guidelines as a basis for indoor air quality standards but with a 1-hour averaging time, as the 24 hours of the WHO AQG is much longer than people usually spend in public places.”
Professor Morawska said mechanical ventilation systems should remove and dilute human-emitted and other indoor-generated pollutants at a higher rate than their production so that they would not accumulate in indoor air.
“The technologies for measuring ventilation already exist in most modern mechanically ventilated buildings but monitoring ventilation rates in terms of clean air delivered to the space requires us to consider the number of people and their activities in the space to ensure adequate IAQ.
“A practical ventilation standard could be air from outside (assumed to be clean), or clean recirculated air to the entire occupied zone and with airflow not directed from one person to another.
“Additional measures in support of ventilation, such as air cleaning and disinfection, could greatly reduce the need to increase the outdoor air supply, which carries a heavy energy demand.
“Filtering recirculated air is an effective way to reduce concentration of, and thus our exposure to, airborne particulate matter, allergens and pathogens.”
Mandating indoor air quality standards in public buildings was published in Science.
The expert contributors were Professor Morawska, Professor Belinda Bennett, and Professor Amanda Kennedy, QUT, Australia; Associate Professor Joseph Allen, Harvard University, USA; Professor William Bahnfleth, The Pennsylvania State University, USA; Professor Philomena M. Bluyssen and Professor Atze Boerstra, Delft University of Technology, The Netherlands; Professor Giorgio Buonanno, University of Cassino and Southern Lazio, Cassino, Italy; Professor Junji Cao, Chinese Academy of Science, China; Professor Stephanie J. Dancer, Edinburgh Napier University, UK; Professor Andres Floto and Dr Charles Haworth, University of Cambridge, UK; Francesco Franchimon, Franchimon ICM, The Netherlands; Professor Trish Greenhalgh, University of Oxford, UK; Jaap Hogeling, International Standards at ISSO, The Netherlands; Associate Professor Christina Isaxon and Associate Professor Aneta Wierzbicka, Lund University, Sweden; Professor Jose L. Jimenez and Professor Shelly L. Miller, University of Colorado, USA; Professor Prashant Kumar, University of Surrey, UK; Professor Jarek Kurnitski, Tallinn University of Technology, Estonia; Professor Yuguo Li, University of Hong Kong, China; Associate Professor Marcel Loomans, Eindhoven University of Technology, The Netherlands; Professor Guy Marks, University of New South Wales; Professor Linsey C. Marr,Virginia Tech, USA, Professor Livio Mazzarella, Politecnico di Milano, Italy; Professor Arsen Krikor Melikov and Professor Pawel Wargocki, Technical University of Denmark, Denmark; Professor Donald K. Milton, University of Maryland; Professor Jason Monty, University of Melbourne, Australia; Associate Professor Peter V. Nielsen, Aalborg University, Denmark; Professor Catherine Noakes, University of Leeds, UK; Professor Jordan Peccia, Yale University, USA; Professor Kimberly A. Prather, University of California, USA; Professor Xavier Querol, Institute of Environmental Assessment and Water Research, Spain; Professor Tunga Salthammer, Fraunhofer WKI, Germany; ProfessorChandra Sekharand Associate Professor Kwok Wai Tam, National University of Singapore, Singapore; Associate Professor Olli Seppänen, Aalto University Finland; Professor Shin-ichi Tanabe, Waseda University, Japan; Associate ProfessorJulian W. Tang, University of Leicester, UK; Associate Professor Raymond Tellier, McGill University, Canada; Professor Maosheng Yao,, Peking University, China.
RNA-based immunizing agents have enriched the repertoire of technologies used for vaccine development. An analysis of the active clinical trials in early…
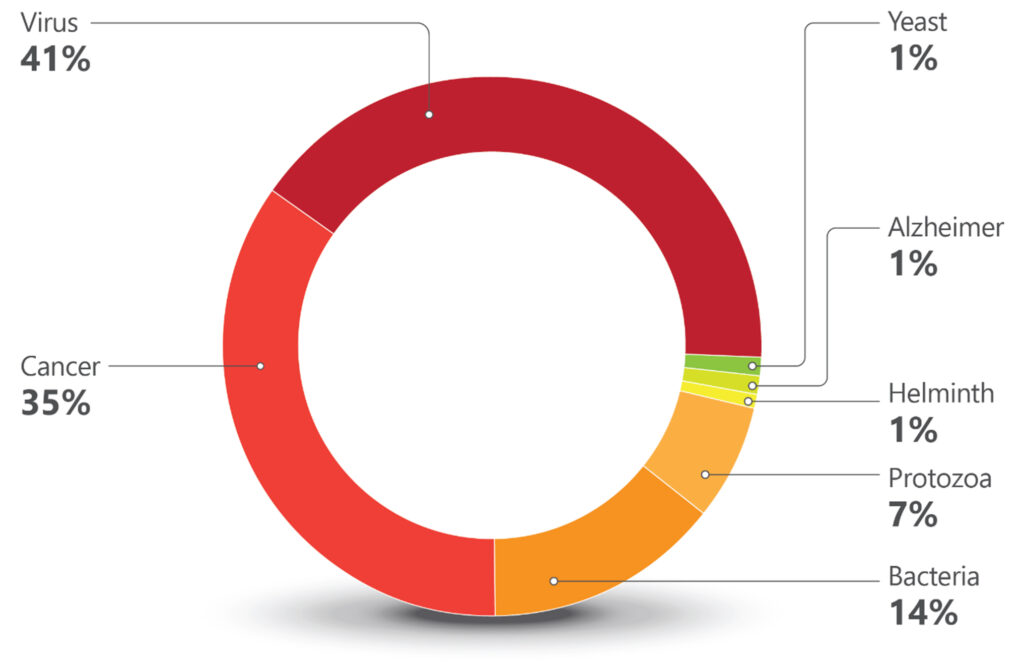
RNA-based immunizing agents have enriched the repertoire of technologies used for vaccine development. An analysis of the active clinical trials in early Phase I and Phase I during the year of 2023 illustrates this point. A total of 161 active vaccine trials were registered at clinicaltrials.gov. Information from these trials was used to plot (Chart 1) and (Chart 2) SARS-CoV-2/COVID-19 trials were excluded to give more evidence to other disease targets.
Chart 1. Targets for Vaccines in Early Stages of Clinical Development. Early Phase I and Phase I clinical trials were grouped according to the diseases (cancer or Alzheimer) or type of infectious agents (viruses, bacteria, protozoa, helminth, and yeast). One-hundred-sixty-one trials were identified using vaccine as keyword and filters for active trials and therapeutic intervention during the period of 01/01/2023 to 1/7/2024. COVID 19/SARS-CoV-2 related trials were excluded. [clinicaltrials.gov]The highest number of trials were against viral infections (67 trials). Most have influenza, Herpes zoster, RSV (Respiratory Syncytial virus), and HIV as targets. The commercially available flu vaccines do need improvement and RNA technologies provide hope for better products. Different companies are exploring this space, including Moderna, Sanofi, Pfizer, Arcturus, Seqirus, and GSK.
The commercial success of Shingrix®, the GSK vaccine against Herpes zoster, has led to five companies in China to follow suit with their own products. Moderna is also pursuing the shingles market with an mRNA-based candidate, while Immorna (China) is testing a self-replicating RNA vaccine. Another competitive market is vaccines for respiratory tract infections. RSV is the leading causative agent for lower track respiratory diseases, causing 3.4 million hospitalizations and 950,00–150,000 deaths every year.
Until recently, no vaccines against the virus were commercially available, but two were approved by the FDA in 2023. Arexvy® from GSK, was approved for older adults, and Abrysvo® from Pfizer, for adults and pregnant women (to protect infants from birth to six months). Four other companies are developing vaccines against RSV.
Blue Lake Biotechnology (U.S.) and Codagenix (U.S.) are testing pediatric vaccines. The former is working on an intranasal recombinant parainfluenza virus type 5 for infants and children, and the latter, also developing an intranasal pediatric vaccine, but based on a live-attenuated engineered virus. Sanofi has two trials, one for infants (intranasal) based on live attenuated virus and one for adults (intramuscular) against both RSV and hMPV (human metapneumovirus).
Targeting both these viruses in one jab is also in Moderna’s and AstraZeneca’s pipeline. While Moderna is developing an mRNA-based formulation for infants, AstraZeneca, through the acquisition of Icosavax, has a VLP (Virus-Like Particle) platform technology with a lead program targeting both viruses[1].
Decades of difficulties in the development of vaccines against HIV resulted in many companies dropping their research programs targeting the virus. Of the eight ongoing trials, seven are sponsored by research institutions and only one is sponsored by a company, Vir Biotechnology.
Second largest target
The second largest target in number of trials is cancer (56 trials). The vast majority involve the development of immunotherapies and a recurrent approach are therapeutic vaccines using dendritic cells loaded with personalized neoantigens. Ten out of the 56 cancer trials are based on RNA technologies. Nature’s publication from June 2023[2], showing promising results of a personalized neoantigen mRNA immunotherapy for pancreatic cancer, indicated the feasibility of this complex approach.
The number of companies as sponsors of early-stage trials for vaccines for cancer is smaller than that for viral infections (many cancer trials are sponsored by research/academic institutions). Nevertheless, a good proportion of the company-sponsored trials are for cancers associated with viruses, such as is the case for the HPV vaccines. The vast majority of cervical cancers is associated with the presence of the HPV virus and immunization programs almost eliminated cervical cancer in women born in England since 1995[3].
It is reasonable to hope that the vaccines being developed for EBV (Epstein–Barr virus) or CMV (Cytomegalovirus) associated cancers (hematological malignancies and glioblastomas, respectively) can be successful as well. Immunomic Therapeutics has a DNA formulation based on its UNITE® proprietary technology that explores the CMV-GBM association.
The twelve trials in the protozoa group (Chart 1) are all against just one protozoan, Plasmodium, the causative agent of malaria. Six are sponsored by the University of Oxford. R21, the vaccine developed by Oxford University and the Serum Institute of India, is based on a recombinant protein. It is the second vaccine recommended by the WHO for malaria, a fusion recombinant product which is part circumsporozoite protein of Plasmodium falciparum and part Hepatitis B surface protein antigen.
Recombinant construct
Expressed in yeast, this recombinant construct is more immunogenic and cheaper to manufacture than Mosquirix® (the first malaria vaccine recommended by WHO, developed by GSK)[4]. It is worthy to note that all formulations in University of Oxford’s trials employ the Matrix-MTM adjuvant, which was developed by Novavax and is made with compounds from the bark of the Chilean tree Quillaja saponaria[5].
Twenty trials are registered against bacterial infections: tetanus, diphtheria, Shigellosis, pneumococcal, streptococcal, and meningococcal infections, tuberculosis, and Lyme Disease are the targets. Old unmet medical needs, such as Lyme disease and tuberculosis, are being addressed (also) by mRNA technologies. The Austrian company Eveliqure has a new approach for attenuating genetically engineered bacteria and is testing its oral ShigETEC against Shigellosis. In Australia, GPN Vaccines innovated on inactivation of whole organisms and is using its technology against pneumococcal infections.
Chart 2. Technologies Used for Vaccine Development. [Golgher and Rodrigues]Lastly are the trials that comprise a low percentage of the pipeline, which is unfortunate since they address unmet medical needs of millions. There is just one trial against helminths, against schistosomiasis, a disease that affects 240 million people. Sponsored by the International Vaccine Institute, it has Seattle-based PAI Life Sciences as a collaborator.
Two trials are against Alzheimer disease, both sponsored by research institutions. One is a DNA based vaccine that aims to elicit antibodies against amyloid-β.The other, interestingly, is testing if the BCG vaccine (Bacillus Calmette–Guérin) has an effect on reducing biomarkers for the disease. BCG vaccines are based on attenuated forms of the bacterium Mycobacterium bovis.
The only trial against a fungal infection targets yeast. The goal is to generate protection for women who experience recurrent vulvovaginal candidiasis, and the trial is sponsored by the Swiss company LimmaTech Biologics, in collaboration with GSK. There are no available vaccines against fungal infections, which are responsible for an annual global death rate of approximately 1.5 million[6].
More input needed from South America
Interesting points could be drawn from the analysis of the ongoing early Phase I and Phase I clinical trials on vaccines. There were more European biotechnology companies (11) (Austria, Denmark, France, Germany, Switzerland, Sweden) plus one in the U.K., than there were American companies (10).
By adding the Australian and Asian companies in early stages clinical trials, there were 30 biotechs dedicated to the development of interesting immunizing agents. By mix and matching old approaches (inactivated or attenuated) with more modern ones (recombinant proteins, fusion constructs, VLPs, RNA, DNA), using systems biology, genetic engineering, AI), innovation in vaccines is flourishing. See Figure 1.
Figure 1. Novel, and not so novel, technologies incrementing the vaccine pipeline. [Golgher and Rodrigues]Some of the diseases studied by the companies developing these early-stage clinical trials are predominantly health problems of low- and middle-income countries. It is disappointing to note the absence of companies from South America among the sponsors or collaborators in these trials. According to IQVIA, the global vaccine market (excluding COVID-19) reached $39 billion in 2022, with a growth rate of seven percent CAGR between 2017–2022[7]. The market is mostly driven by innovative vaccines and is bound to grow. South American countries must work to have a better share of it.
Brazil has an admirable vaccination program and internationally recognized governmental vaccine factories (Butantan and Biomanguinhos), but a poor track record on innovation in this area[8]. It is senseless to invest so much in the training of excellent immunologists, vaccinologists, and infectious disease experts and not translate this into novel products. A lot more can be done.
If it depends on the initiative, CTVacinas (soon to be CN Vaccines, CN for National Center), coordinated by the researcher Ricardo Gazzinelli, DSc, DVM, Oswaldo Cruz Foundation and Universidade Federal de Minas Gerais (UFMG), it will be done.
For those who know Gazzinelli, it is easy to bet that the enterprise under his leadership, which includes the collaboration of several other researchers from UFMG, will thrive. When it comes to partnerships, CTVacinas is open and agnostic; what matters is that meaningful projects move forward, and partners can come from private, public, international or national institutions. An important part of their mission is to be an institute good at translating academic research into novel immunizing formulations. The aim is to generate more businesses, products, and startups.
CTVacinas has a history: part of its revenues come from royalties from a vaccine for dogs against visceral leishmaniasis, developed by Gazzinelli and his business partner, Ana Paula Fernandes.
Figure 2. Ricardo Gazzinelli, pictured on the right and the CTVacinas team on the left. CTVacinas is located at UFMG’s technology park, it is a leading organization in developing vaccine projects that can become innovative products and businesses. The initiative has secured funds for expansion. [CTVacinas]In CTVacinas pipeline is SpiN-Tec, a vaccine against SARS-CoV-2, now in Phase II trials. It is the first 100% Brazilian vaccine. SpiN-Tec is a made of a recombinant fusion product of the S and N proteins of the virus, and the hope is that it will confer protection irrespective of the strain.
Helton Santiago, MD, PhD, a professor at UFMG who works with Gazzinelli, is responsible for SpiN-Tec’s clinical program, among others. He is an enthusiastic member of the CTVacinas vaccine team and is optimistic about the future of Brazil in the vaccine field. According to Santiago, the COVID-19 pandemic stimulated the national players to move at a faster pace toward innovation.
If some needed a pandemic to shake them out of a sluggish mode, others have started out going as fast as possible. It is the case, for example, of Luana Raposo, Bruna Porchia, and Mariana Diniz, founders of ImunoTera, a spinoff from the University of São Paulo (Figure 3). With proprietary technology developed during their PhDs, they have succeeded in securing funds for their company’s first steps.
Figure 3. Founders of ImunoTera, Luana Raposo (left) and Bruna Porchia (right) at the Albert Einstein Hospital. ImunoTera was one of the startups selected for the hospital’s biotechnology program. [Tauan Sousa]ImunoTera is dedicated to developing immunotherapies against infectious diseases and cancer and has been selected for competitive preincubation and incubation programs in the country. The founders have chosen wisely and, with the support of the best programs and partners to develop their pipeline, are advancing. Their first product has been tested in patients with HPV-induced high grade cervical neoplasia, with promising results. ImunoTera may be the one to develop the next 100% Brazilian vaccine.
Denise Golgher, PhD (d.golgher@gmail.com) is a life sciences consultant based in São Paulo, Brazil. Rob Rodrigues, LLM, Stanford Law School, is a partner at Licks Attorneys. Many thanks to our interviewees, Luana Raposo from Imunotera, Walderez Dutra from UFMG, Ricardo Gazzinelli and Helton Santiago from CT vacinas, Eduardo Levi from DASA, Jorge Kalil from USP and Constantino Lopez from Instituto Mexicano del Seguro Social.
LOS ANGELES — A clinical trial from Keck Medicine of USC will test the feasibility of treating non-small cell lung cancer with immunotherapy provided at home.
Credit: Ricardo Carrasco III
LOS ANGELES — A clinical trial from Keck Medicine of USC will test the feasibility of treating non-small cell lung cancer with immunotherapy provided at home.
Immunotherapy, medicines that use the body’s immune system to eliminate or control cancer cells, are effective for many cancer patients, but are currently only administered intravenously (into the vein) in a doctor’s office or hospital.
The study will examine if a new formulation of atezolizumab, an immunotherapy approved for treating certain types of non-small cell lung cancer, can instead be safely and effectively administered subcutaneously, meaning it is injected under the patient’s skin, by a nurse at the patient’s home, along with telemedicine appointments and remote monitoring through wearable trackers.
This will be the first clinical trial to test at-home administration of subcutaneous immunotherapy and could potentially lay the foundation for the future of at-home cancer care.
“Many types of drugs are now being delivered subcutaneously at home for several conditions, and we hypothesize that this method of drug delivery can also be successful for cancer patients,” said Jorge Nieva, MD, a medical oncologist and lung cancer specialist with Keck Medicine, a member of USC Norris Comprehensive Cancer Center and lead investigator of the clinical trial. “Additionally, since COVID-19, we’ve learned that physicians have the digital tools to provide patients with excellent remote care.”
The benefits of at-home treatment
Lung cancer is the second most diagnosed cancer in the world and the leading cause of cancer deaths for both men and women worldwide. Non-small cell lung cancer accounts for 81% of all lung cancer cases in the United States.
Immunotherapy is a relatively new treatment option that has been approved to treat many cancer types both on its own or in combination with other therapies, such as radiation and chemotherapy.
Nieva believes that moving immunotherapy from a medical setting to the home will benefit patients. Patients will save time and energy traveling to a clinic or doctor’s office, which can be especially difficult for those who are very sick, and they may feel more relaxed in their own homes. This could also potentially expand access to cancer treatment to patients who live in more remote areas or lack reliable access to transportation.
Delivering the drug under the skin rather than through an intravenous line (IV) has advantages as well.
“The procedure is easier and faster to administer and less likely to cause infection or complications, and patients avoid the potential discomfort of being stuck with a needle several times in the attempt to find a suitable vein for the IV,” said Nieva.
Nieva was motivated to research at-home cancer treatments during the COVID-19 pandemic when a patient who was afraid of catching the virus died after he stopped going into the hospital for his cancer treatments.
“I realized we had to change the delivery of cancer care,” said Nieva.
Clinical trial will use an immunotherapy consisting of monoclonal antibodies
The drug used in the clinical trial, atezolizumab, consists of a monoclonal antibody, a man-made protein that triggers the immune system to attack cancer cells. It was approved by the Food and Drug Administration in 2016 for late-stage lung cancer and more recently in 2021, for early stage, non-small cell lung cancer.
Investigators aim to enroll 37 patients with non-small cell lung cancer who are deemed eligible to receive immunotherapy as treatment. Patients will receive treatments administered by a nurse who will visit their home every three weeks for one to two years.
Additionally, Nieva and his colleagues will use the latest digital tools to track patients’ vital signs, physical activity and other markers of health remotely and monitor patients with telehealth visits.
The study will not only examine the feasibility of home administration of the medication, but how well patients comply with the program and how satisfied they are with being treated remotely and through telehealth appointments.
Nivea hopes that the clinical trial will not only benefit patients with non-small cell lung cancer, but other cancer patients as well.
“Increasingly, health care is moving in a direction where instead of patients going to us for services, we are able to come to them, increasing access to care and potentially addressing existing health care disparities,” said Nieva. “If this study can show that at-home cancer immunotherapy is safe and feasible for non-small cell lung cancer, it will open the door for more home treatments for other types of cancers in the future.”
To learn more about the criteria to participate in the clinical trial, click here. Those who are interested in participating in the trial may contact Sandy Tran at (323) 865-3935 or sandy.tran@med.usc.edu.
The sponsors of the clinical trial are the National Cancer Institute (NCI), grant number ML43326, and Genentech, Inc.
###
For more information about Keck Medicine of USC, please visit news.KeckMedicine.org.
Walgreens Incurs $5.8Bn Charge on VillageMD Amid Cost-Cutting
Under the leadership of CEO Rosalind Brewer, the company sought to enhance its healthcare offerings by investing heavily in VillageMD, a network of doctors’…
Under the leadership of CEO Rosalind Brewer, the company sought to enhance its healthcare offerings by investing heavily in VillageMD, a network of doctors’ clinics known for consuming substantial cash flows.
Over recent years, Walgreens has poured more than $6 billion into acquiring a majority stake in VillageMD, further bolstering its healthcare footprint with a $3.5 billion investment in Summit Health in 2022.
However, a strategic pivot occurred with Timothy Wentworth stepping in as the new CEO, bringing a sharpened focus on bolstering profitability. This included unveiling a comprehensive plan to trim costs by $1 billion in October as part of a broader effort to realign the company’s financial strategies.
This quarter, the repercussions of these investments became starkly evident as Walgreens reported a net loss of $5.9 billion for the quarter ending February 29, primarily due to the significant impairment charge. Concurrently, the company adjusted its profit outlook for the 2024 fiscal year downwards, reflecting the ongoing economic pressures impacting its retail segment.
This revision sets a more conservative benchmark for growth expectations in the 2025 fiscal year, as Leerink Partners analyst Michael Cherny noted. This amplifies concerns about Walgreens’ fundamental earning capabilities.
Amid these challenges, Walgreens also contends with diminished consumer spending on personal care and beauty items, a trend exacerbated by inflation and a decline in demand for COVID-19 vaccines and testing services. This broader consumer reticence has further strained the company’s financial performance, evidenced by a 1.4% drop in premarket shares.
Despite these hurdles, Walgreens managed to surpass analyst expectations on an adjusted basis, posting earnings of $1.20 per share for the quarter against the consensus forecast of 82 cents per share from LSEG data.
The company has revised its adjusted earnings projection for the fiscal year ending August 31 to between $3.20 and $3.35 per share. It maintains the lower end of its initial January forecast while narrowing the upper limit from the previously stated $3.50 per share.
We use cookies on our website to give you the most relevant experience by remembering your preferences and repeat visits. By clicking “Accept”, you consent to the use of ALL the cookies.
This website uses cookies to improve your experience while you navigate through the website. Out of these, the cookies that are categorized as necessary are stored on your browser as they are essential for the working of basic functionalities of the website. We also use third-party cookies that help us analyze and understand how you use this website. These cookies will be stored in your browser only with your consent. You also have the option to opt-out of these cookies. But opting out of some of these cookies may affect your browsing experience.
Necessary cookies are absolutely essential for the website to function properly. These cookies ensure basic functionalities and security features of the website, anonymously.
Cookie
Duration
Description
cookielawinfo-checbox-analytics
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Analytics".
cookielawinfo-checbox-functional
11 months
The cookie is set by GDPR cookie consent to record the user consent for the cookies in the category "Functional".
cookielawinfo-checbox-others
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Other.
cookielawinfo-checkbox-necessary
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookies is used to store the user consent for the cookies in the category "Necessary".
cookielawinfo-checkbox-performance
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Performance".
viewed_cookie_policy
11 months
The cookie is set by the GDPR Cookie Consent plugin and is used to store whether or not user has consented to the use of cookies. It does not store any personal data.
Functional cookies help to perform certain functionalities like sharing the content of the website on social media platforms, collect feedbacks, and other third-party features.
Performance cookies are used to understand and analyze the key performance indexes of the website which helps in delivering a better user experience for the visitors.
Analytical cookies are used to understand how visitors interact with the website. These cookies help provide information on metrics the number of visitors, bounce rate, traffic source, etc.
Advertisement cookies are used to provide visitors with relevant ads and marketing campaigns. These cookies track visitors across websites and collect information to provide customized ads.