International
Getting the balance right
Even as their clients are trying to make clinical trials more diverse and equitable, agencies are continuing their DE&I efforts to build a culture…
Share this:

Getting the balance right
Even as their clients are trying to make clinical trials more diverse and equitable, agencies are continuing their DE&I efforts to build a culture where diverse talent is welcomed.
By Christiane Truelove • chris.truelove@medadnews.com
If there is a “positive” side to the COVID-19 pandemic, it is how the crisis illuminated the deep differences in the quality of healthcare in communities of color in the United States. From access to medicines to how pharmaceutical companies recruit for their clinical trials, pharma knows it has some work to do.
The development of COVID-19 vaccines highlighted not only the importance of clinical trials but the need to diversify them. However, there remains a barrier. Because of barbarities such as the Tuskegee syphilis experiment – the most well known, but certainly not the only incident of abuse posing as medical science – there remains a deep distrust by PoC about participating in clinical trials. And these feelings of distrust are deepened by socioeconomic and healthcare inequities.
Driving efforts to diversify the population of clinical trials – at least when it comes to those in the United States – is the Food and Drug Administration. In April 2020, FDA issued a new draft guidance to the life sciences industry for developing plans to enroll more participants from underrepresented racial and ethnic populations into clinical trials. The guidance, titled “Diversity Plans to Improve Enrollment of Participants from Underrepresented Racial and Ethnic Subgroups in Clinical Trials,” recommends that sponsors of medical products develop and submit a Race and Ethnicity Diversity Plan to the agency early in clinical development, based on a framework outlined in the guidance.
“The U.S. population has become increasingly diverse, and ensuring meaningful representation of racial and ethnic minorities in clinical trials for regulated medical products is fundamental to public health,” stated FDA Commissioner Robert M. Califf, M.D. “Going forward, achieving greater diversity will be a key focus throughout the FDA to facilitate the development of better treatments and better ways to fight diseases that often disproportionately impact diverse communities. This guidance also further demonstrates how we support the Administration’s Cancer Moonshot goal of addressing inequities in cancer care, helping to ensure that every community in America has access to cutting-edge cancer diagnostics, therapeutics and clinical trials.”
Among the barriers identified by FDA about minority participation in clinical trials are mistrust of the clinical research system due to historical abuses; aspects of the trial design such as inadequate recruitment and retention efforts, frequency of study visits; time and resource constraints for participants; and transportation and participation conflicting with caregiver or family responsibilities.
Additional barriers could be language and cultural differences, health literacy, religion, limited access within the healthcare system, and a lack of awareness and knowledge about what a clinical trial is and what it means to participate.
“The FDA remains committed to increasing enrollment of diverse populations in medical product and drug development and will continue to engage with federal partners, medical product manufacturers, healthcare professionals and health advocates to reach this important goal,” officials stated.
In addition to the guidance, FDA’s Office of Minority Health and Health Equity created the “Diversity in Clinical Trials Initiative,” which includes an ongoing public education and outreach campaign to help address some of the barriers preventing diverse groups from participating in clinical trials. The office’s dedicated webpage has public service announcements and videos, social media outreach, and other resources such as infographics (“4 Ways to Be a Clinical Trials Champion”), a brochure (“Research Needs You”), and a fact sheet.
Industry actions for DE&I in R&D
While FDA has made some deliberate moves to encourage diversity in clinical trials, industry has been thinking about the problem for some time. TransCelerate BioPharma Inc. is a coalition of 20 pharmaceutical companies with “a vision consisting of healthcare providers (HCPs) that are activated and supporting patients along their healthcare and clinical research journey, where HCPs, sites and investigative staff are fully supported by trial sponsors, researchers have access to the data they need to improve study design, and medications are developed faster for patients in need.”
TransCelerate’s member companies are AbbVie, Amgen, Astellas, AstraZeneca, Bayer, Boehringer Ingelheim, Bristol Myers Squibb, Merck KGaA, GSK, Johnson & Johnson, Lilly, MSD, Novartis, Novo Nordisk, Pfizer, Regeneron, Roche, Sanofi, Shionogi, and UCB.
According to TransCelerate, there are R&D inefficiencies around approaches and processes for drug development. These have caused roadblocks for successfully starting, recruiting, executing, and completing clinical research studies, ultimately delaying the development of needed medications for patients.
There is a very practical reason for manufacturers to promote diversity in clinical trials, TransCelerate executives say. Not only does a lack of diversity lead to persistent gaps between trial representation and real-world disease burden, underrepresentation can limit confidence in future approved therapies and could lead to unforeseen consequences among impacted patient populations.
In 2014, TransCelerate launched its Diversity of Participants in Clinical Trials initiative, which executives believe will help accelerate improvements by equipping trial sponsors and other stakeholders with the tools and resources they need.
On its website, TransCelerate’s tools to promote diversity in clinical trials include “Diversity Community-Based Site Engagement and Capacity Building,”which identifies areas that clinical trial sponsors can make improvements; “Sponsor Toolkit Site Engagement and Capacity Building Considerations for Diversity, Equity and Inclusion of Participants in Clinical Trials (DEICT)”; and a reference table of available resources. These include BIOEquality, the Center for Information and Study on Clinical Research Participation (CISCRP), and the National Minority Quality Forum (NMQF).

Jeneen Donadeo, executive director, portfolo solutions at TransCelerate
Jeneen Donadeo, executive director, portfolo solutions at TransCelerate, says the distrust pharma continues to experience about clinical trial participation is a “human” challenge, but one companies must be willing to take on. And as far as raising awareness of clinical trials, “I think the pandemic has helped us with that in a very odd way. Prior to COVID, how many people really gave much thought about research and development of medicines? If they took an aspirin or ibuprofen, were they thinking about, ‘Oh, I wonder how this was made? And who volunteered to make it and who was involved?’”
Post-COVID drug development is still probably a mystery to some people, but Donadeo says, “There’s more awareness now that [drug development is] there; it is something that needs to happen. And it does need participants – it’s not magically happening somewhere in a vacuum without the participation of humans in the process.”
Right now, one of the biggest challenges is access – how the industry can help to get the right participants into the right trials, Donadeo says. “One of the problems we’re seeing in so many diseases, is access to health care, access to the best health care, whether that is clinical trials or not – but clinical trials being part of that conversation,” she says.
For any patient, no matter what their background, the person that can help them make a decision to go into a clinical trial is their trusted healthcare provider. But when TransCelerate polled HCPs a few years ago about getting their patients into clinical trials, the organization found “in some cases, it’s not even on the radar [for HCPs] to recommend clinical research,” Donadeo says.
TransCelerate believes that more work needs to be done with HCPs to raise awareness of clinical trials, especially in communities of color.
“I think there is a ton of work to do in that whole trust piece, around how you get patients access to the trials, and how you get them relating to someone that you trust to help them make the decisions, and that has the right information to help them make that decision,” Donadeo says.
Based on these findings, TransCelerate has been focusing over the past year on efforts to equip clinical trial sponsors with better information about how to overcome the challenges of working with some sites.
Donadeo says there is no easy solution to the challenges of diversifying clinical trials, but in the end it has to be all stakeholders working together. “It’s not just pharma alone,” she says.
In October, Genentech released a video called “Question Reality,” part of its “Ask Bigger Questions” campaign on racial equity in health care. The video depicts the story of a Black woman throughout her journey with the healthcare system, first as a patient and later as an empowered Genentech scientist and leader. As a young girl, she questions why a doctor didn’t believe her, and as an industry-leader, she stresses the importance of asking bigger questions and addressing the root causes of systemic inequities in health care. The film was directed by Courtney Sofiah Yates, a Brooklyn-based and award-winning Black filmmaker and photographer.

Veronica Sandoval, principal, inclusion and health equity, Genentech
“It is time that as an industry, we back up our words with intentional actions that tackle the root causes of systemic healthcare inequities,” states Veronica Sandoval, principal, inclusion and health equity, Genentech. “This crisis is not new. Barriers to access and quality health care have had generational impacts and have taken the lives of far too many people. Through this new campaign, ‘Question Reality,’ Genentech aims to elevate important questions that often go unheard and ignite a sense of urgency to address them.”
Sandoval told Med Ad News that while the ongoing COVID-19 pandemic has exacerbated health inequity and widened the gap for underrepresented communities, “the problems we are seeing run deeper than just those brought on by COVID-19.
“At Genentech, we are actively working to dismantle systemic racism, which is a root cause of many health disparities and has contributed to poorer health outcomes for people of color and other marginalized communities. Our commitment includes tackling specific problems brought on by COVID-19, but is not limited to those issues.”
According to Sandoval, the “Ask Bigger Questions” campaign is not Genentech’s first and only initiative to advance health equity.
“We have also launched marketing and education initiatives to address the complex health inequities for Black and Hispanic/Latinx people with MS, who make up a combined 35 percent of the MS population, but account for only 13 percent of the population being treated today,” she says. “For example, we have developed and launched culturally relevant, multi-channel education, access solutions and support including Spanish direct-to-consumer (DTC) advertising and an #MSVisibility campaign centering [on] the experiences of Hispanic/Latinx MS patients.”
While Genentech is trying to encourage an industry-wide movement for health equity, the company continues to focus on its own efforts.
“As the pioneers of the biotech industry, we have an opportunity and responsibility to use our resources to build deep and sustainable partnerships with stakeholders across the healthcare ecosystem to make health equity a reality for all patients,” Sandoval told Med Ad News. “Genentech is uniquely resourced and positioned to have systemic impact within our company and beyond.
“Health equity is core to Genentech’s mission and strategy, and we seek to integrate a focus on equity in everything we do – from the design of clinical studies, to our access and policy priorities, to our investments in the community. We are committed to a health equity strategy that puts historically excluded patients at the center of what we do, and to fostering a healthcare ecosystem that earns the trust of and is accountable to all communities.”
According to Sandoval, Genentech has redesigned new clinical trials to accommodate more diverse populations. More than five years ago, the company implemented Advancing Inclusive Research, a cross-
functional effort aimed at addressing barriers and reducing disparities in clinical research participation for underrepresented racial and ethnic groups. Since then Genentech has launched the Advancing Inclusive Research Site Alliance and founded and partnered with its External Council for Inclusive Research to establish new standards and principles for inclusive research.
Since 2017, Genentech has invested more than $125 million in giving towards health equity and diversity in STEM-focused giving and national partnerships. And the company has conducted several clinical trials prioritizing the recruitment of historically underrepresented and excluded patient populations with a focus on diseases that disproportionately impact these communities.
“Together, we are sharing our key learnings with the industry at-large,” Sandoval says. “We recently published a peer-reviewed manuscript that included system, study, and patient level recommendations to improve the diversity of patient enrollment in clinical research.”
Trials that Genentech has redesigned to become more diversified include EMPACTA, CHIMES, and ELEVATUM.
EMPACTA (Evaluating Minority Patients with Actemra) study is a Phase III trial for patients hospitalized with COVID-19 pneumonia. The study was designed in collaboration with physicians at hospitals with diverse patient populations, creating a streamlined process to identify and perform outreach. “Data shows that Black and Hispanic/Latinx patients have been disproportionately impacted by hospitalizations and mortality from COVID-19,” Sandoval states. “By meeting patients in their own communities, we were able to enroll 389 participants in under one month – 84 percent of whom were from underrepresented groups.”
CHIMES focuses on Black and Hispanic/Latinx patients with relapsing-remitting multiple sclerosis. The goal of the study is to optimize the protocol and simplify logistics to make participation as convenient as possible.
“As a result, the team put into place several interventions to remove barriers to participation, including on-demand transportation services, a patient stipend program, and culturally competent patient education materials,” Sandoval says. “These efforts helped the CHIMES team exceed its target, enrolling nearly 170 patients – 100 percent of whom are Black or Hispanic/Latinx – more than two months ahead of schedule.”
ELEVATUM is a post-approval study in USMA to understand the safety and efficacy of Faricimab in Black and Hispanic/Latinx diabetic macular edema patients.
“From the study’s inception, the ELEVATUM team used guidance from both CHIMES and EMPACTA to focus on design elements that will remove barriers to participation among underrepresented patient groups,” Sandoval says.
These elements will include door-to-door transportation service free of cost to the low- vision patients participating participants in the study, as well as stipends to compensate participants for the three-to four-hour imaging assessments that are required during visits.
“All therapeutic areas can benefit from more diverse clinical trial populations, but focusing on diseases that disproportionately impact underrepresented communities will drive forward a more equitable health system,” Sandoval told Med Ad News.
Beyond clinical trial access, Genentech is committed to ensuring that its medicines get to the people who need them, even if they can’t afford them. According to Sandoval, over the past 30 years, Genentech has helped more than three million people get the medicine they need through patient assistance programs such as Genentech Access Solutions and the Genentech Patient Foundation.
Genentech Access Solutions helps patients and their providers understand their healthcare benefits and insurance coverage and can help direct them to appropriate assistance programs based on their situation and need. “In 2021, we helped more than 255,000 people access the Genentech medicines they needed,” Sandoval says.
The Genentech Patient Foundation provides free Genentech medicine for eligible patients who do not have insurance or who have insurance but have been denied coverage or where their out-of-pocket costs are still unaffordable. Sandoval states that last year, Genentech provided free medicine to more than 60,000 people.
Expanding on the Genentech Patient Foundation’s mission to advance health equity, the company has initiated the CA & OR Latinx Farmworker Outreach Project, which aims to gain a deeper understanding of the access barriers that Latino farmworker communities in California and Oregon face, and connect with regional organizations in order to support access to free medicine.
In California, 92 percent of farmworkers are Latino, and most farmworkers – 53 percent – have no health insurance and limited access to healthcare, making them particularly vulnerable to environmental and occupational health hazards.
“In 2020 we launched our first Health Equity Study to elevate the perspectives and experiences of historically marginalized patient populations,” Sandoval says. “In 2021, we probed deeper and found that both patients and healthcare providers agree that the healthcare system needs urgent reform. By publishing the data from these stories and elevating the experiences of medically disenfranchised patients, we hope to spark action to address inequities across the healthcare ecosystem.
“We launched and published the study to amplify the voices of patients often forgotten, or talked about but not talked with/asked to engage in the conversation. Since then we continue to dedicate our resources and invest in initiatives that center the experience and voices of marginalized patients.”
Pfizer, Med Ad News’ 2022 Company of the Year, has taken a visible stance on clinical trial diversity. The company published a study in the July 2021 issue of Contemporary Clinical Trials, “Demographic diversity of participants in Pfizer sponsored clinical trials in the United States.”
The purpose of the study was to summarize the race, ethnicity, gender, and age data for Pfizer’s trials in the United States between 2011 and 2020. The results were used to establish a baseline of clinical trial diversity to measure improvement over time.
Pfizer analyzed the data set, comprising 213 trials with 103,103 U.S. participants, and found that overall trial participation of Black or African American individuals was at the U.S. census level (14.3 percent vs. 13.4 percent). Participation of Hispanic or Latino individuals was below U.S. census levels (15.9 percent vs. 18.5 percent), and female participation was at U.S. census levels (51.1 percent vs. 50.8 percent).
The analysis also examined what percentage of trials achieved racial and ethnic distribution levels at or above census levels. Participant levels above census were achieved in 56.1 percent of Pfizer trials for Black or African American participants, 51.4 percent of trials for White participants, 16 percent of trials for Asian participants, 14.2 percent of trials for Native Hawaiian and Pacific Islander participants, 8.5 percent of trials for American Indian and Alaska Native participants, and 52.3 percent of trials for Hispanic or Latino participants.
In its blog posting about the results of this study – “Doing Better: Increasing Diversity in Clinical Trials” – Pfizer admitted that White people are over-represented in therapeutic trials, or those in which the treatment under investigation is likely to benefit trial participants in some way. 78.6 percent of therapeutic trial participants were White; 17 percent were Black and just 2.2 percent were Asian.
While more than half of Pfizer trials included Black participants at rates about equal to their representation in the overall population, Black people were under-
represented in cancer-related studies. Only about 16 percent of oncology studies included proportional representation of Black people, Pfizer executives say.
And Hispanic or Latino individuals are particularly underrepresented in cancer-related studies, with just 6.5 percent of oncology trials including proportional representation of Hispanic or Latino people.
Pfizer also found that Native Hawaiian, Pacific Islander, and Indigenous populations were under-represented, with some trials failing to include any individuals from these demographic groups.
“Volunteering to participate in a clinical trial – the foundation of medical research – is a selfless and personal choice that is often a challenge for many communities due to societal and economic factors,” stated Dara Richardson-Heron, M.D., Pfizer’s former chief patient officer. “Pfizer’s goal is to partner with patients’ and patient advocates to co-create solutions designed to lower many of the known barriers to clinical trial research such as financial challenges, lack of accessibility, the digital divide and many others. Pfizer must also do its part to increase awareness about the value and benefits of research and nurture relationships that will rebuild trust in our nation’s healthcare system.”
Pfizer says it has taken decisive steps toward eliminating healthcare equity barriers, including a company-wide commitment to diversity and knowledge
-sharing. “For clinical trials themselves, in some cases, researchers may cover participants’ travel expenses and utilize available digital technology to minimize (or eliminate) onerous on-site visits,” executives say, adding that Pfizer will also emphasize partnering with local clinics and grassroots organizations, and listening to the needs and concerns of individuals in the community.
“Overcoming barriers and challenges to fair representation won’t happen overnight, nor can it be achieved by a single company,” MacKenzie stated. “But it is the right thing to do for science, for public health, and for patients who are waiting for the next breakthrough.”
The continuing agency efforts of DE&I

Walt Geer, chief experience officer, VMLY&R
Healthcare advertising agencies continue to focus on their DE&I efforts, but their work, and the work of their clients, has really just begun, executives say.
“We’ve all gotten past the easy part, which was simply having the conversations,” says Walter T Geer III, chief experience design officer at VMLY&R Health. “But now, the hard part is actually doing the work.”
Geer told Med Ad News that for smaller organizations, creating diversity is easy, but for other larger ones, it will be more difficult. “We [VMLY&R and VMLY&R Health] have almost 14,000 employees; I think we’re doing an incredible job,” he says. “But it’s also something that I would assume many people understand that it’s not a job that can be done overnight.”
Part of the work that needs to be done in diversity “is simply about ensuring that you have the right voices and the right individuals, and right ethnicities and backgrounds, on the work both in front of the camera and behind the camera,” Geer says.
He says VMLY&R has a culture studio, the job of which is to be able to talk about different areas of culture, areas that some people might not be comfortable with. “That’s important; [it] shows that we’re dedicated to getting the work done correctly.”
One of the barriers to doing any DE&I work is fear. “While many want to do the work, there’s a bit of fear of, ‘Well, if I do this, is it going to be wrong? And then oh, my gosh, I don’t want to get canceled,’” Geer told Med Ad News. “Then there’s the thought of, ‘Well, let’s just not do it at all, because we don’t want to get ourselves in trouble.’”
With the prevalence of social media, “we’re presented with a very difficult moment in time, because of the power of one individual sitting in their bedroom anywhere, being able to make a comment that has a potential of going viral and making a brand look bad,” Geer says.
On the positive side, Geer notes that over the past three years, VMLY&R’s health partners have had more people of color on the other side of the screen.
Geer attributes this to the shift in perception about the importance of pharma companies in the wake of the COVID-19 pandemic. “If you said to anyone three years ago, that a pharma company would be the most well known brand in the world, everyone would say, ‘Hell no.” Because the first thing you’d think of are brands like Nike.”
With Pfizer and other pharma companies coming into the limelight, “I think that pharma brands had to rethink how they go to market, rethink what their story is,” Geer says.
As the pandemic highlights the health inequities for people of color, pharma has realized “getting it right means truly saving lives, and getting some of that wrong means we’re letting a vast amount of society down, and people could die over this stuff,” Geer says. “So pharma companies need to get it right, and have to get it right, and understand that getting it right means involving everyone, right to the table.”
This means a pharma company can’t have a table of six men trying to create a product for women with menstrual cycle problems – just as agencies “can’t have six people sit in a room as we try to solve a problem for a particular type of disability that none of us have,” Geer says. “It’s ensuring that you have a multitude of voices in these rooms. And we’re most certainly starting to see more of that now on the pharma side.”
For agencies and their pharma clients, the biggest challenge remains creating a culture that welcomes diversity, according to Geer. One of the difficulties in doing that is culture tends to conform to the norms of the majority. “People want to go to a place where they feel comfortable, and that means you’re going to a place where you have people that are similar to you – similar ways of thinking, similar way of walking, and talking and style, and all of that.”
This means it’s simply not enough to make diverse hires. “I’m kind of happy that we’ve gotten past the moment of, let’s talk about our DE&I numbers, because DE&I numbers, to me, don’t really mean anything,” Geer told Med Ad News. “I think that when an organization is leading with their diversity numbers, that is essentially saying, ‘Okay, so I’m buying my way into fixing this problem.’”
The solution to the problem is creating culture, Geer stated. “When I walk into an office, I can tell you in less than five minutes if this company is diverse or not.”
So how can a company create a diverse culture? The first step is finding the right talent. “The [healthcare advertising] industry as a whole needs to do a better job of identifying talent and where they pull the talent from,” Geer says.
Many tech companies excel because they don’t emphasize a tech background with prospective talent, “they could care less that you work in an agency at a publisher or a brand. They just want to find the talent,” Geer says. “Agencies, for a long time, all of us have felt as though finding the right talent means finding someone else who’s worked in an agency, because they have to get an agency environment and how agencies work.”
Geer himself has only been in the agency space for three and a half years. “And I will tell you, it is a challenge,” he says. “I’m still learning on a daily basis how a lot of this functions and works. It is an uphill challenge.
“But bringing in someone like I am, [with] an entirely different background from someone that you would typically see in my type of role at an agency – VMLY&R Health understood that was being disruptive. Being able to bring different and unique or inventive solutions and ideas means we need to bring different types of people to the table to execute on that.
“We just can’t rotate the same talent, it means pulling externally and looking at different types of individuals to bring to the table.”

Tope Ajala, global head of diversity, equity, and inclusion at Ogilvy
Tope Ajala, global head of diversity, equity, and inclusion at Ogilvy, says for agencies and other organizations, getting that diversity of people is a talent war, which is being driven by how people feel they belong in an organization.
“So I always tell my team, representation creates communities, and communities stick together,” Ajala says. “So if you see a mass exodus of a specific group of people from your organization, they don’t feel like they belong, and they aren’t being represented fully.
“We’re realizing that communities really are a thing. Representation creates community, and we need to see more representation across all of our industry, whether that’s health, whether that’s advertising as a whole, and just whether that’s even within our leadership, [or] your organizational structure, how are you representing the people you want to come in house? And if you’re not representing them, then you’re not going to get them.”
According to Ajala, too often HR people are looking for prospective employees who are a culture fit, but in reality, are just “mini versions” of themselves.
“What we should be looking for is a ‘culture add’,”she says. “Is this person actually very different from us? Can they deliver the work? And most times, nine or 10 times actually, yes, they can deliver the work, so the right candidate you want to hire, the challenging part comes with, we will have natural biases.”
In assembling her own teams, Ajala says she has tried to go outside of her own experiences, to find people who not just complement the overall corporate culture, but who can add to it. Someone who is Muslim or Latinx, for example, would bring perspectives she does not possess.
“The more we learn about the differences people have, the more we start creating a better culture where anyone can come and thrive, and where anyone feels like they belong,” Ajala says.

Michelle Edwards, VP of operations and human resources at Heartbeat
Michelle Edwards, VP of operations and human resources at Heartbeat, says in building the agency’s culture, executives “are relentlessly in pursuit” of creating a Heartbeat community that mirrors the demographics of New York City, where the agency is based.
“We have a ways to go to be able to get the same statistics, breakdown demographics wise, in New York, but those are our big goals, to be able to match those same demographics.”
Geer notes that for pharma companies dealing with trying to reach patients of color, another problem that frequently pops up is authenticity.
“Number one is understanding that authenticity is everything,” he says. “And authenticity means understanding who you are, and understanding when to interject yourself into conversation, and when involving yourself in that conversation, knowing that it’s not to be speaking at people, but how to speak with them.”
Joining a conversation late “looks like you’re just trying to jump on the bandwagon,” Geer says, adding that achieving this understanding is difficult for pharma brands to do.
Geer believes that pharma can use tech to help bridge gaps. Partnering with tech companies such as Google or Amazon or Apple, all of whom have devices that patients are using to communicate in real time, can help pharma tap into those connected conversations and experiences and make health care more accessible.
At present, though, “When we get involved in clinical trials, there’s a significant amount of people who still don’t trust because of years of mistreatment,” Geer says. “And again, getting there, being able to do that appropriately, it’s the messenger that matters. Who’s delivering that message? Is it a pastor or a trusted individual?
“And most certainly, when you see brands that are trying to, diversify their clinical trials, because they understand the importance, you see then people on the other side of things going, ‘Nah, I don’t want to, I don’t trust that.’”
Another factor to contend with is that the HCPs who should be acting as the trusted intermediaries between patients and pharma and clinical trials may be operating under erroneous race-based assumptions.
“There are still doctors being trained today with misinformation like Black people have thicker skin and not as many nerves, [and] they have a higher pain tolerance – it’s crazy,” Geer says.
Five years ago, Geer experienced one of those doctors when he had an accident during a cycling race. “I cut my whole knee open, and the doctor literally said, ‘Oh, you’re a big, tough guy, we don’t need to give you any anesthesia.’ And he literally started sewing my knee up without any anesthesia.”
Pharma companies need to start diversifying their KOLs early in the product development process. “It is about tapping into the communities, and diversifying your teams and ensuring you have people on a consultative level who are sitting side by side along the entire process,” Geer says.
Ajala is passionate about DE&I because of the complexity of her own reality. “I’m British, born of German and Nigerian parents, now living in the United States,” Ajala says. “But when I first moved to the U.S., I was seen as African American, that was the first thing everyone saw, until they heard me speak. So automatically, you’re judged based off of your skin complexion, and where you’re located, forgetting that people obviously come from different walks of life.”
Wherever Ajala has lived – London, Dubai, Singapore, Germany, the United States – “my skin color is still the first thing I’m judged on. And that becomes the most challenging thing that I have to live with. And that shouldn’t be the case.”
For Ajala, the attitudes toward her that she has seen in the world are replicated in the workplace. “We hear these conversations around, you know, diversity matters, inclusion matters. We’re doing a lot about it. But are we really?”
DE&I programs can help an organization become more successful, “because people want to be where they see themselves.
“If representation is lacking in your business, it is going to fail,” Ajala says, “And there’s tons of examples around multiculturalism and how we market to different groups. But by eliminating and ignoring certain groups, you lose a seat.”
After the awareness of racial inequities was raised by the murder of George Floyd, Ajala noted with interest the number of articles that came out educating about DE&I.
“We weren’t comfortable in 2020, which is what I loved, which forced businesses to look inward and think about how they could change their industry specifically,” Ajala says, with pharma companies asking themselves questions about whether study data and pilot groups were reflective of the people they actually were trying to target.
“The question is, in 2022, have we kept the momentum going?” Ajala says. “And I’m afraid the answer is ‘no’ for most organizations.”
Like Geer, Ajala has seen fear slowing DE&I efforts. “[DE&I] makes people feel incredibly uncomfortable,” she says. “And I think you had no choice in 2020. It was in your face 24/7, and we were stuck at home.”
For leaders currently, Ajala says, “now that the uncomfortability is not in your face every day,” the challenge is to keep that DE&I momentum going, “to ensure that it’s still being spoken about in corridors, in meetings, with clients, with patients, with friends, with family.”
Edwards says one of the many ways Heartbeat keeps DE&I conversations going is though education. For example, the agency has a historian come in on a regular basis to teach about less well known aspects of events such as the assassinations of Malcolm X and John F. Kennedy, or about the slave trade and the destruction of Tulsa’s “Black Wall Street.”
“We felt like just knowing our history, it helps you realize where we are and how we got here,” Edwards says. “And it helps to understand what are the things that we need to do to move forward.”
And for Heartbeat, though Edwards is proud of the achievements of the agency’s employee groups such as the Dismantling Racism group, “what got us to where we are is the foundation that we’ve built on how our leaders make decisions, how our leaders interact with people, how we all treat each other, how we communicate with each other, how we celebrate one another, how we collaborate, and how we support each other,” Edwards says. “[That] was the key to get to where we are, and all those things I talk about kind of exist on top of, in addition to, and because of that strong foundation.”
Without that kind of leadership and communication as a foundation, other companies may falter in their DE&I progress, Edwards notes.
Having Black History Month celebrations and other sorts of activities “is really low-hanging fruit type things,” she says. “A lot of companies, they just go straight to those things. But you really have to start with the foundation. And that’s really a mindset shift.”
 |
Chris Truelove is contributing editor of Med Ad News and PharmaLive.com. |
International
President Biden Delivers The “Darkest, Most Un-American Speech Given By A President”
President Biden Delivers The "Darkest, Most Un-American Speech Given By A President"
Having successfully raged, ranted, lied, and yelled through…
Share this:

Having successfully raged, ranted, lied, and yelled through the State of The Union, President Biden can go back to his crypt now.
Whatever 'they' gave Biden, every American man, woman, and the other should be allowed to take it - though it seems the cocktail brings out 'dark Brandon'?
Tl;dw: Biden's Speech tonight ...
-
Fund Ukraine.
-
Trump is threat to democracy and America itself.
-
Abortion is good.
-
American Economy is stronger than ever.
-
Inflation wasn't Biden's fault.
-
Illegals are Americans too.
-
Republicans are responsible for the border crisis.
-
Trump is bad.
-
Biden stands with trans-children.
-
J6 was the worst insurrection since the Civil War.
(h/t @TCDMS99)
Tucker Carlson's response sums it all up perfectly:
"that was possibly the darkest, most un-American speech given by an American president. It wasn't a speech, it was a rant..."
Carlson continued: "The true measure of a nation's greatness lies within its capacity to control borders, yet Bid refuses to do it."
"In a fair election, Joe Biden cannot win"
And concluded:
“There was not a meaningful word for the entire duration about the things that actually matter to people who live here.”
Victor Davis Hanson added some excellent color, but this was probably the best line on Biden:
"he doesn't care... he lives in an alternative reality."
— Tucker Carlson (@TuckerCarlson) March 8, 2024
* * *
Watch SOTU Live here...
* * *
Mises' Connor O'Keeffe, warns: "Be on the Lookout for These Lies in Biden's State of the Union Address."
On Thursday evening, President Joe Biden is set to give his third State of the Union address. The political press has been buzzing with speculation over what the president will say. That speculation, however, is focused more on how Biden will perform, and which issues he will prioritize. Much of the speech is expected to be familiar.
The story Biden will tell about what he has done as president and where the country finds itself as a result will be the same dishonest story he's been telling since at least the summer.
He'll cite government statistics to say the economy is growing, unemployment is low, and inflation is down.
Something that has been frustrating Biden, his team, and his allies in the media is that the American people do not feel as economically well off as the official data says they are. Despite what the White House and establishment-friendly journalists say, the problem lies with the data, not the American people's ability to perceive their own well-being.
As I wrote back in January, the reason for the discrepancy is the lack of distinction made between private economic activity and government spending in the most frequently cited economic indicators. There is an important difference between the two:
-
Government, unlike any other entity in the economy, can simply take money and resources from others to spend on things and hire people. Whether or not the spending brings people value is irrelevant
-
It's the private sector that's responsible for producing goods and services that actually meet people's needs and wants. So, the private components of the economy have the most significant effect on people's economic well-being.
Recently, government spending and hiring has accounted for a larger than normal share of both economic activity and employment. This means the government is propping up these traditional measures, making the economy appear better than it actually is. Also, many of the jobs Biden and his allies take credit for creating will quickly go away once it becomes clear that consumers don't actually want whatever the government encouraged these companies to produce.
On top of all that, the administration is dealing with the consequences of their chosen inflation rhetoric.
Since its peak in the summer of 2022, the president's team has talked about inflation "coming back down," which can easily give the impression that it's prices that will eventually come back down.
But that's not what that phrase means. It would be more honest to say that price increases are slowing down.
Americans are finally waking up to the fact that the cost of living will not return to prepandemic levels, and they're not happy about it.
The president has made some clumsy attempts at damage control, such as a Super Bowl Sunday video attacking food companies for "shrinkflation"—selling smaller portions at the same price instead of simply raising prices.
In his speech Thursday, Biden is expected to play up his desire to crack down on the "corporate greed" he's blaming for high prices.
In the name of "bringing down costs for Americans," the administration wants to implement targeted price ceilings - something anyone who has taken even a single economics class could tell you does more harm than good. Biden would never place the blame for the dramatic price increases we've experienced during his term where it actually belongs—on all the government spending that he and President Donald Trump oversaw during the pandemic, funded by the creation of $6 trillion out of thin air - because that kind of spending is precisely what he hopes to kick back up in a second term.
If reelected, the president wants to "revive" parts of his so-called Build Back Better agenda, which he tried and failed to pass in his first year. That would bring a significant expansion of domestic spending. And Biden remains committed to the idea that Americans must be forced to continue funding the war in Ukraine. That's another topic Biden is expected to highlight in the State of the Union, likely accompanied by the lie that Ukraine spending is good for the American economy. It isn't.
It's not possible to predict all the ways President Biden will exaggerate, mislead, and outright lie in his speech on Thursday. But we can be sure of two things. The "state of the Union" is not as strong as Biden will say it is. And his policy ambitions risk making it much worse.
* * *
The American people will be tuning in on their smartphones, laptops, and televisions on Thursday evening to see if 'sloppy joe' 81-year-old President Joe Biden can coherently put together more than two sentences (even with a teleprompter) as he gives his third State of the Union in front of a divided Congress.
President Biden will speak on various topics to convince voters why he shouldn't be sent to a retirement home.
The state of our union under President Biden: three years of decline. pic.twitter.com/Da1KOIb3eR
— Speaker Mike Johnson (@SpeakerJohnson) March 7, 2024
According to CNN sources, here are some of the topics Biden will discuss tonight:
Economic issues: Biden and his team have been drafting a speech heavy on economic populism, aides said, with calls for higher taxes on corporations and the wealthy – an attempt to draw a sharp contrast with Republicans and their likely presidential nominee, Donald Trump.
Health care expenses: Biden will also push for lowering health care costs and discuss his efforts to go after drug manufacturers to lower the cost of prescription medications — all issues his advisers believe can help buoy what have been sagging economic approval ratings.
Israel's war with Hamas: Also looming large over Biden's primetime address is the ongoing Israel-Hamas war, which has consumed much of the president's time and attention over the past few months. The president's top national security advisers have been working around the clock to try to finalize a ceasefire-hostages release deal by Ramadan, the Muslim holy month that begins next week.
An argument for reelection: Aides view Thursday's speech as a critical opportunity for the president to tout his accomplishments in office and lay out his plans for another four years in the nation's top job. Even though viewership has declined over the years, the yearly speech reliably draws tens of millions of households.
Sources provided more color on Biden's SOTU address:
The speech is expected to be heavy on economic populism. The president will talk about raising taxes on corporations and the wealthy. He'll highlight efforts to cut costs for the American people, including pushing Congress to help make prescription drugs more affordable.
Biden will talk about the need to preserve democracy and freedom, a cornerstone of his re-election bid. That includes protecting and bolstering reproductive rights, an issue Democrats believe will energize voters in November. Biden is also expected to promote his unity agenda, a key feature of each of his addresses to Congress while in office.
Biden is also expected to give remarks on border security while the invasion of illegals has become one of the most heated topics among American voters. A majority of voters are frustrated with radical progressives in the White House facilitating the illegal migrant invasion.
It is probable that the president will attribute the failure of the Senate border bill to the Republicans, a claim many voters view as unfounded. This is because the White House has the option to issue an executive order to restore border security, yet opts not to do so
Maybe this is why?
Most Americans are still unaware that the census counts ALL people, including illegal immigrants, for deciding how many House seats each state gets!
— Elon Musk (@elonmusk) March 7, 2024
This results in Dem states getting roughly 20 more House seats, which is another strong incentive for them not to deport illegals.
While Biden addresses the nation, the Biden administration will be armed with a social media team to pump propaganda to at least 100 million Americans.
"The White House hosted about 70 creators, digital publishers, and influencers across three separate events" on Wednesday and Thursday, a White House official told CNN.
Not a very capable social media team...
The State of Confusion https://t.co/C31mHc5ABJ
— zerohedge (@zerohedge) March 7, 2024
The administration's move to ramp up social media operations comes as users on X are mostly free from government censorship with Elon Musk at the helm. This infuriates Democrats, who can no longer censor their political enemies on X.
Meanwhile, Democratic lawmakers tell Axios that the president's SOTU performance will be critical as he tries to dispel voter concerns about his elderly age. The address reached as many as 27 million people in 2023.
"We are all nervous," said one House Democrat, citing concerns about the president's "ability to speak without blowing things."
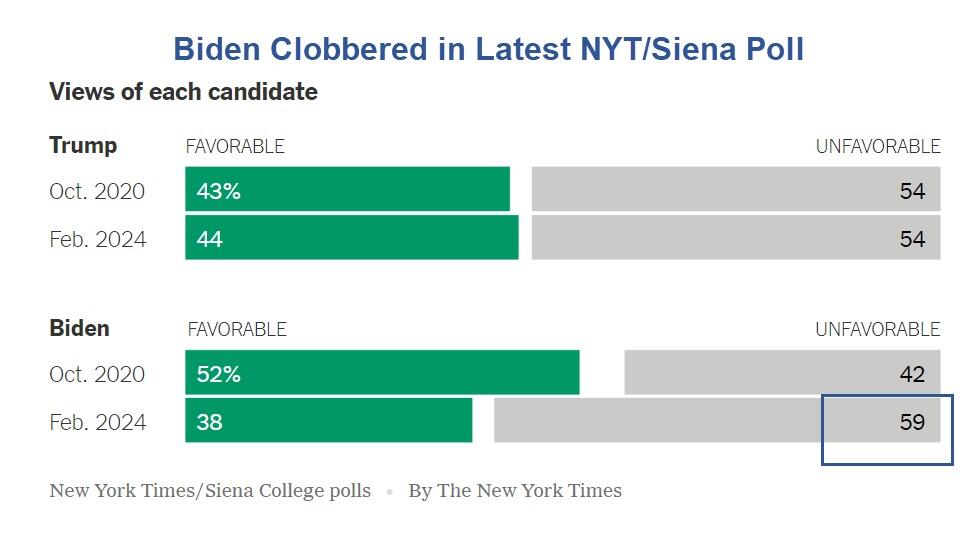
The SOTU address comes as Biden's polling data is in the dumps.
BetOnline has created several money-making opportunities for gamblers tonight, such as betting on what word Biden mentions the most.
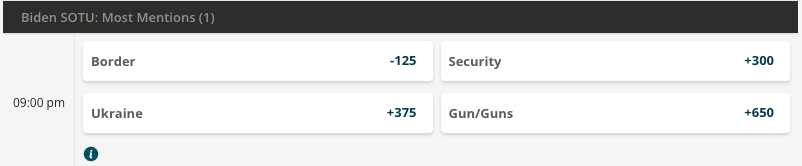
As well as...
We will update you when Tucker Carlson's live feed of SOTU is published.
Fuck it. We’ll do it live! Thursday night, March 7, our live response to Joe Biden’s State of the Union speech. pic.twitter.com/V0UwOrgKvz
— Tucker Carlson (@TuckerCarlson) March 6, 2024
International
What is intersectionality and why does it make feminism more effective?
The social categories that we belong to shape our understanding of the world in different ways.
Share this:


The way we talk about society and the people and structures in it is constantly changing. One term you may come across this International Women’s Day is “intersectionality”. And specifically, the concept of “intersectional feminism”.
Intersectionality refers to the fact that everyone is part of multiple social categories. These include gender, social class, sexuality, (dis)ability and racialisation (when people are divided into “racial” groups often based on skin colour or features).
These categories are not independent of each other, they intersect. This looks different for every person. For example, a black woman without a disability will have a different experience of society than a white woman without a disability – or a black woman with a disability.
An intersectional approach makes social policy more inclusive and just. Its value was evident in research during the pandemic, when it became clear that women from various groups, those who worked in caring jobs and who lived in crowded circumstances were much more likely to die from COVID.
A long-fought battle
American civil rights leader and scholar Kimberlé Crenshaw first introduced the term intersectionality in a 1989 paper. She argued that focusing on a single form of oppression (such as gender or race) perpetuated discrimination against black women, who are simultaneously subjected to both racism and sexism.
Crenshaw gave a name to ways of thinking and theorising that black and Latina feminists, as well as working-class and lesbian feminists, had argued for decades. The Combahee River Collective of black lesbians was groundbreaking in this work.
They called for strategic alliances with black men to oppose racism, white women to oppose sexism and lesbians to oppose homophobia. This was an example of how an intersectional understanding of identity and social power relations can create more opportunities for action.
These ideas have, through political struggle, come to be accepted in feminist thinking and women’s studies scholarship. An increasing number of feminists now use the term “intersectional feminism”.
The term has moved from academia to feminist activist and social justice circles and beyond in recent years. Its popularity and widespread use means it is subjected to much scrutiny and debate about how and when it should be employed. For example, some argue that it should always include attention to racism and racialisation.
Recognising more issues makes feminism more effective
In writing about intersectionality, Crenshaw argued that singular approaches to social categories made black women’s oppression invisible. Many black feminists have pointed out that white feminists frequently overlook how racial categories shape different women’s experiences.
One example is hair discrimination. It is only in the 2020s that many organisations in South Africa, the UK and US have recognised that it is discriminatory to regulate black women’s hairstyles in ways that render their natural hair unacceptable.
This is an intersectional approach. White women and most black men do not face the same discrimination and pressures to straighten their hair.

“Abortion on demand” in the 1970s and 1980s in the UK and USA took no account of the fact that black women in these and many other countries needed to campaign against being given abortions against their will. The fight for reproductive justice does not look the same for all women.
Similarly, the experiences of working-class women have frequently been rendered invisible in white, middle class feminist campaigns and writings. Intersectionality means that these issues are recognised and fought for in an inclusive and more powerful way.
In the 35 years since Crenshaw coined the term, feminist scholars have analysed how women are positioned in society, for example, as black, working-class, lesbian or colonial subjects. Intersectionality reminds us that fruitful discussions about discrimination and justice must acknowledge how these different categories affect each other and their associated power relations.
This does not mean that research and policy cannot focus predominantly on one social category, such as race, gender or social class. But it does mean that we cannot, and should not, understand those categories in isolation of each other.
Ann Phoenix does not work for, consult, own shares in or receive funding from any company or organisation that would benefit from this article, and has disclosed no relevant affiliations beyond their academic appointment.
africa uk pandemicGovernment
Biden defends immigration policy during State of the Union, blaming Republicans in Congress for refusing to act
A rising number of Americans say that immigration is the country’s biggest problem. Biden called for Congress to pass a bipartisan border and immigration…
Share this:

{kind=link}
{kind=link}

President Joe Biden delivered the annual State of the Union address on March 7, 2024, casting a wide net on a range of major themes – the economy, abortion rights, threats to democracy, the wars in Gaza and Ukraine – that are preoccupying many Americans heading into the November presidential election.
The president also addressed massive increases in immigration at the southern border and the political battle in Congress over how to manage it. “We can fight about the border, or we can fix it. I’m ready to fix it,” Biden said.
But while Biden stressed that he wants to overcome political division and take action on immigration and the border, he cautioned that he will not “demonize immigrants,” as he said his predecessor, former President Donald Trump, does.
“I will not separate families. I will not ban people from America because of their faith,” Biden said.
Biden’s speech comes as a rising number of American voters say that immigration is the country’s biggest problem.
Immigration law scholar Jean Lantz Reisz answers four questions about why immigration has become a top issue for Americans, and the limits of presidential power when it comes to immigration and border security.

1. What is driving all of the attention and concern immigration is receiving?
The unprecedented number of undocumented migrants crossing the U.S.-Mexico border right now has drawn national concern to the U.S. immigration system and the president’s enforcement policies at the border.
Border security has always been part of the immigration debate about how to stop unlawful immigration.
But in this election, the immigration debate is also fueled by images of large groups of migrants crossing a river and crawling through barbed wire fences. There is also news of standoffs between Texas law enforcement and U.S. Border Patrol agents and cities like New York and Chicago struggling to handle the influx of arriving migrants.
Republicans blame Biden for not taking action on what they say is an “invasion” at the U.S. border. Democrats blame Republicans for refusing to pass laws that would give the president the power to stop the flow of migration at the border.
2. Are Biden’s immigration policies effective?
Confusion about immigration laws may be the reason people believe that Biden is not implementing effective policies at the border.
The U.S. passed a law in 1952 that gives any person arriving at the border or inside the U.S. the right to apply for asylum and the right to legally stay in the country, even if that person crossed the border illegally. That law has not changed.
Courts struck down many of former President Donald Trump’s policies that tried to limit immigration. Trump was able to lawfully deport migrants at the border without processing their asylum claims during the COVID-19 pandemic under a public health law called Title 42. Biden continued that policy until the legal justification for Title 42 – meaning the public health emergency – ended in 2023.
Republicans falsely attribute the surge in undocumented migration to the U.S. over the past three years to something they call Biden’s “open border” policy. There is no such policy.
Multiple factors are driving increased migration to the U.S.
More people are leaving dangerous or difficult situations in their countries, and some people have waited to migrate until after the COVID-19 pandemic ended. People who smuggle migrants are also spreading misinformation to migrants about the ability to enter and stay in the U.S.

3. How much power does the president have over immigration?
The president’s power regarding immigration is limited to enforcing existing immigration laws. But the president has broad authority over how to enforce those laws.
For example, the president can place every single immigrant unlawfully present in the U.S. in deportation proceedings. Because there is not enough money or employees at federal agencies and courts to accomplish that, the president will usually choose to prioritize the deportation of certain immigrants, like those who have committed serious and violent crimes in the U.S.
The federal agency Immigration and Customs Enforcement deported more than 142,000 immigrants from October 2022 through September 2023, double the number of people it deported the previous fiscal year.
But under current law, the president does not have the power to summarily expel migrants who say they are afraid of returning to their country. The law requires the president to process their claims for asylum.
Biden’s ability to enforce immigration law also depends on a budget approved by Congress. Without congressional approval, the president cannot spend money to build a wall, increase immigration detention facilities’ capacity or send more Border Patrol agents to process undocumented migrants entering the country.

4. How could Biden address the current immigration problems in this country?
In early 2024, Republicans in the Senate refused to pass a bill – developed by a bipartisan team of legislators – that would have made it harder to get asylum and given Biden the power to stop taking asylum applications when migrant crossings reached a certain number.
During his speech, Biden called this bill the “toughest set of border security reforms we’ve ever seen in this country.”
That bill would have also provided more federal money to help immigration agencies and courts quickly review more asylum claims and expedite the asylum process, which remains backlogged with millions of cases, Biden said. Biden said the bipartisan deal would also hire 1,500 more border security agents and officers, as well as 4,300 more asylum officers.
Removing this backlog in immigration courts could mean that some undocumented migrants, who now might wait six to eight years for an asylum hearing, would instead only wait six weeks, Biden said. That means it would be “highly unlikely” migrants would pay a large amount to be smuggled into the country, only to be “kicked out quickly,” Biden said.
“My Republican friends, you owe it to the American people to get this bill done. We need to act,” Biden said.
Biden’s remarks calling for Congress to pass the bill drew jeers from some in the audience. Biden quickly responded, saying that it was a bipartisan effort: “What are you against?” he asked.
Biden is now considering using section 212(f) of the Immigration and Nationality Act to get more control over immigration. This sweeping law allows the president to temporarily suspend or restrict the entry of all foreigners if their arrival is detrimental to the U.S.
This obscure law gained attention when Trump used it in January 2017 to implement a travel ban on foreigners from mainly Muslim countries. The Supreme Court upheld the travel ban in 2018.
Trump again also signed an executive order in April 2020 that blocked foreigners who were seeking lawful permanent residency from entering the country for 60 days, citing this same section of the Immigration and Nationality Act.
Biden did not mention any possible use of section 212(f) during his State of the Union speech. If the president uses this, it would likely be challenged in court. It is not clear that 212(f) would apply to people already in the U.S., and it conflicts with existing asylum law that gives people within the U.S. the right to seek asylum.
Jean Lantz Reisz does not work for, consult, own shares in or receive funding from any company or organization that would benefit from this article, and has disclosed no relevant affiliations beyond their academic appointment.
congress senate trump pandemic covid-19 mexico ukraine

EyePoint poaches medical chief from Apellis; Sandoz CFO, longtime BioNTech exec to retire


Redefining Poverty: Towards a Transpartisan Approach


The Digest #187


Gather ’round the crystal ball: A multi-commodity outlook from PDAC 2024


Is “Greedflation” Over?


Catastrophic Risk: Investing and Business Implications


Deterra Royalties half-yearly result: stable performance and growth Initiatives


Deflationary pressures in China – be careful what you wish for


Is the United States overestimating China’s power?


Stock Market Today: Tech leads gains, S&P 500, Gold at record highs
-

 Uncategorized2 weeks ago
Uncategorized2 weeks agoAll Of The Elements Are In Place For An Economic Crisis Of Staggering Proportions
-

 Uncategorized1 month ago
Uncategorized1 month agoCathie Wood sells a major tech stock (again)
-

 Uncategorized3 weeks ago
Uncategorized3 weeks agoCalifornia Counties Could Be Forced To Pay $300 Million To Cover COVID-Era Program
-

 Uncategorized2 weeks ago
Uncategorized2 weeks agoApparel Retailer Express Moving Toward Bankruptcy
-

 Uncategorized3 weeks ago
Uncategorized3 weeks agoIndustrial Production Decreased 0.1% in January
-

 International1 month ago
International1 month agoWar Delirium
-

 Uncategorized3 weeks ago
Uncategorized3 weeks agoRFK Jr: The Wuhan Cover-Up & The Rise Of The Biowarfare-Industrial Complex
-

 Uncategorized3 weeks ago
Uncategorized3 weeks agoGOP Efforts To Shore Up Election Security In Swing States Face Challenges