Government
Fight Like a Mother: When an ICD-10 Code Determines Life or Death
By Frieda Wiley Treating chronic illnesses usually saves lives. However, when that condition lacks a billing code, seeking treatment can become a death…
Share this:

By Frieda Wiley
Treating chronic illnesses usually saves lives. However, when that condition lacks a billing code, seeking treatment can become a death sentence. At least that’s what doctors told Amber Freed, a 43-year-old mother of two who learned that something seemingly as trivial as a billing code could become a life-or-death situation.
It all began shortly after Freed gave birth to fraternal twins Maxwell and Riley in March 2017. The newly found joys of motherhood quickly transformed into fear after she observed marked differences between her two children’s developmental progression.
“I noticed Riley was advancing faster than Maxwell,” she said, “[Maxwell] had strange movements, his eyes were open, and he didn’t know his name,” she recalls.
He also felt different in her arms. “He felt floppy to me compared to Riley.”
Freed could easily fill Riley’s baby book with fun memories and important milestones. Meanwhile, Maxwell’s book lacked a similar narrative and remained largely empty.
Maternal instincts trump a doctor’s experience
Worried, the new mother took her son to his pediatrician, who immediately dismissed her concerns. He assured her Maxwell was progressing normally, telling her that girls develop faster than boys. Still, Freed could not shake the feeling that something was wrong. Her gnawing gut instinct prompted her to schedule an appointment at the Children’s Hospital in Denver, Colorado, where the family lived. There, Maxwell saw a variety of specialists, including an ophthalmologist who gave Freed some startling news after conducting an eye exam on Maxwell.
“His eyes are fine, but I think you should be prepared for him not to live,” he told her.
Completely floored, Freed asked the doctor what he had seen in the exam.
“I saw nothing,” the doctor reiterated. “However, I see parents like you all day long searching for answers and thinking something’s wrong with their kids’ eyes when it’s really their brain.”
Her greatest fears now confirmed, Freed struggled to maintain her composure as she prepared to take her son in for additional testing.
The ophthalmologist’s feedback eventually led to a diagnosis she could never have fathomed. Maxwell had an SLC6A1 mutation that causes epilepsy—a condition so rare it had no name, let alone a cure. Lacking a moniker also meant limited funding for research or other supportive services.
In addition to many of these conditions being incurable or lacking sufficient treatments, patients and their families often struggle to pay for treatments at times because no International Classification of Diseases (ICD) codes have been developed for the conditions they face. The World Health Organization has ownership of the ICD codes, which are designed to track morbidity and mortality data. However, the U.S. health insurance industry has commercialized the codes by using them for billing and payment.
As Freed would soon learn, securing medical treatment for the kind of rare disease Maxwell had would prove quite challenging in the U.S. Rare conditions such as Tay-Sachs disease, hereditary hemochromatosis, Wilson’s disease, and cystic fibrosis are all rare conditions with ICD codes recognized by insurance companies for coverage. Yet, these conditions may be more of the exception than the rule. In the U.S., many other diseases the lack billing codes that insurance companies would use to provide financial coverage and reimbursement. The void amplifies a climate where the privatized and commercialized insurance system fragments healthcare coverage as much as the lack of universally available medical records fractures continuity of care.
“If we were living in Europe, Maxwell’s treatment would be covered because of the nationalized medical systems they have there,” she said.
In addition to the rarity of her son’s condition decreasing the chances of insurance coverage, Freed made another startling discovery. Many billing codes covered seemingly bizarre and rare injuries. Yet not a single billing code acknowledged her son’s nameless condition in any way. Lacking a billing code meant insurance would neither pay for nor reimburse any treatment.
“It’s funny,” she said. “There’s an International Classification Code (ICD)-10 for being bitten by a goose, but there’s no code to treat my child for his condition.”
According to the ICD-10.CM, the code, known as W61.51XD, “describes the circumstance of the injury,” if a goose attacks a person. Goose-inflicted injury is one of many billing codes one might not expect to see listed. Other bizarre ICD-10 codes include Y93.J1, which covers neck injuries from playing the piano, and V97.21, which applies to a parachutist involved in an accident. Billing code V91.07XD addresses burns caused by water skiing and 16.V97.33XD describes a “subsequent encounter” of getting sucked into a jet engine. Curiously, Y92.146 describes a “swimming-pool of prison as the place of occurrence of the external cause.”

Pediatric Emergency Medicine physician The American Academy of Pediatrics
According to Jeffrey Linzer, Sr., MD, a pediatric emergency medicine physician representing the American Academy of Pediatrics, the origins of the seemingly bizarre billing codes stem from a very unlikely source: the U.S. Congress.
“Congress directed the Department of Defense to create a distinction between codes for the military versus non-military,” he told Inside Precision Medicine. “In fact, they recommended 10,000 codes.”
It’s all about the Benjamins
As incredulous as it sounds, Freed’s challenges are not unique. Many patients and families of people with rare diseases living in the U.S. face the same challenge.
The National Institutes of Health defines a rare disease as a disease affecting less than 200,000 people living in the U.S. However, rare diseases have a substantially greater collective impact, affecting 25–30 million U.S. residents. Despite the sizeable total population affected, the prognosis looks grim for most of these 10,000-plus rare diseases as only 500 of them have any type of treatment.,
In addition, the few treatments available often prove far more expensive than the average cost of treating more common chronic conditions in the U.S. According to the U.S. Government Accountability Office, costs for treating rare diseases in the U.S. approached nearly $966 billion in 2019.
When a rare disease affects a child, parents and other caregivers must often assume the costs while juggling additional responsibilities of advocating for their patients and the disease itself while becoming both caregivers to the child and educators to medical professionals, the federal government, and other stakeholders. The arduous undertaking has a sizeable impact on the rare disease community as children account for 50% of people diagnosed with a rare disease.3 Disturbingly, three out of ten children diagnosed with a rare disease will die before their fifth birthday.
“The doctors told me, ‘You will become the expert’,” recalled Freed.
The growing list of insurmountable obstacles Freed faced became overwhelming. Doctors told Freed that she would likely have to give up her burgeoning career to devote herself full-time not only to her son’s care but to educating herself—and others—on the condition. She eventually resigned from her position as an equity and research analyst at a financial firm.
Freed’s fastidious search for solutions ultimately led to a partnership with a scientist to develop a gene therapy for her son, but the clinical trial was halted during the COVID-19 pandemic. In the interim, her son has been receiving injections of an off-label therapy called glycerol phenylbutyrate (Ravicti®). While not a cure, it makes Maxwell’s signs and symptoms more manageable.
When the Food and Drug Administration first approved the drug for urea cycle disorder on February 1, 2013, its cost ranged between $250,000 and $290,000 annually. However, the price skyrocketed once doctors began prescribing it off-label to treat Maxwell’s condition. As of early 2024, glycerol phenylbutyrate ranks among the top ten most expensive therapies in the U.S., costing nearly $800,000 annually for its on-label indication.
Even the cheaper option doesn’t run cheap
“The effect of glycerol phenylbutyrate on children with SLC6A1 is compelling,” Zachary Grinspan, MD, a pediatric neurologist at Weill Cornell Medicine in New York City, told Inside Precision Medicine. “[However, the manufacturer], Horizon Therapeutics, did not pursue a new clinical indication, and Amgen’s strategy is unclear.”

pediatric neurologist
Weill Cornell Medicine, New York City
Prescriptive authority allows Grinspan to prescribe glycerol phenylbutyrate, but it does not fill the void of the noticeably absent ICD-10 code from Maxwell’s medical charts. Insurance companies are less likely to cover a drug written for an off-label indication—especially for such a high-dollar drug.
In the meantime, Grinspan aims to get the drug listed in one of the U.S. four drug compendia (i.e., American Hospital Formulary Service-Drug Information [AHFS-DI], Micromedex DrugDEX [DrugDEX], National Comprehensive Cancer Network [NCCN] Drugs, and Biologics, Compendium, and Clinical Pharmacology) to help increase awareness of the drug.
Although a beneficial treatment, the positive effects of glycerol phenylbutyrate therapy wear off after about a year. Much like developing gene therapy for her son, Freed will continue facing the obstacle of footing the six-figure cost.
ICD-10: the rate-limiting step to treatment, access, and potential cures
Unlike many other developed countries with universal healthcare systems, the privatization of insurance contributes to soaring medical costs. This in turn often makes access to care and treatments cost-prohibitive. However, the federal government also plays a role in this narrative as they oversee the ICD-10 codes.
The Centers for Disease Control and Prevention (CDC) is responsible for tracking mortality and morbidity information at a national level and using the data to generate information on disease incidence and prevalence. The process is relatively simple for chronic diseases affecting the masses, such as hypertension or diabetes, as these conditions have ICD-10 codes.
The Centers for Medicaid and Medicare Services, commonly known as CMS, develops and maintains what is known as the International Classification of Diseases, 10th, Revision, Procedure Coding System (ICD-10-PCS). The CMS classifies treatment for diseases, impairments, and injuries for patients who are hospitalized. However, the approval of coding changes and other changes to the ICD-10 coding systems is a collaborative process between the CMS and the CDC’s National Centers for Health Statistics through a body known as the ICD-10 Coordination and Maintenance Committee. This interdepartmental committee meets biannually and accepts modification suggestions from both the public and private sectors.
“There are only two opportunities to apply for the code, and your application may not even be reviewed given that there’s no formal process,” Freed said.
Could another rare disease change the game?
Although many rare diseases remain unassigned, the success of another rare disease may offer a blueprint for successful ICD-10 applications in the rare disease community.
According to data published in 2022, assigning Angelman syndrome an ICD-10 code on October 1, 2018, resulted in a significant uptick in adoption and uptake in the three years following its release. Billed under ICD-10 code Q93.51, a wide variety of clinicians, including pediatric neurologists, geneticists, and developmental-behavioral medicine specialists, now use this code. In addition, the top five healthcare organizations using the billing code gained prescribing privileges at major medical institutions in the U.S., including the Children’s Medical Center Dallas, the Cincinnati Children’s Hospital Medical Center- Community, and Massachusetts General Hospital.
The Angelman syndrome ICD-10 code assignment results give Grinspan hope for a potential strategy to overcome the ICD-10 code void for SLC6A1.
“For people with rare epilepsies, improving epidemiological estimates and clinical descriptions will guide clinical diagnosis and management, support research initiatives, spur pharmaceutical and medical device development, and help families understand these devastating diseases,” Grinspan said. “ICD-10 codes for specific rare epilepsies are foundational for that effort.”
Grinspan further elaborated that the statistical data captured by the CDC helps clinicians prioritize testing when working up new patients and conduct more thorough workups. This enhances their ability to comprehensively evaluate the patient. Robust data therefore enhances the physicians’ ability to diagnose a condition and forecast the patient’s prognosis.
In addition to the ICD-10 code, clinical trials, and funding, physicians need education to improve outcomes
Clinical trials could support treatment and provide more long-term data for diseases as ultra-rare as Maxwell’s. However, clinical trials in children with rare diseases often prove more complex as they require considerations transcending those typically seen in trials for adults. Parents and caregivers often face higher demands in managing the child, observing and helping the children report their signs and symptoms, and sometimes acting as key decision-makers when enrolling a child into a clinical trial.
Historically, commercial sponsors have been less likely to support clinical trials involving child participants than those involving adults. This trend further amplifies cost woes, as pediatric trials may require more study sites and accrue additional costs for coordination. In addition, clinical trials for rare diseases are typically underpowered due to difficulties in recruiting an ample number of participants.
Various other factors inflate the cost of pediatric clinical trials. For example, they may require more time to complete study procedures and specialized (and therefore pricier) laboratory equipment that can accommodate smaller-volume biological samples. Off-label prescribing of treatments occurs much more frequently in pediatric patients, shrinking potential incentives that might entice funders to finance drugs that are already approved for the adult population. These are just a few factors unique to the pediatric population contributing to the already hefty price tags associated with clinical trials.
Pediatric population aside, clinical trials are costly regardless of the number of enrollees or disease state. In addition to population-specific idiosyncrasies, the number of sites, the anticipated number of enrollees, and phases play a factor. Lastly, the cost of the type of therapy (i.e., small molecule versus large molecule, gene therapy, etc.) is a significant factor affecting the total cost.

According to Kimberly Goodspeed, MD, assistant professor in the departments of pediatrics, neurology, and psychiatry at UT Southwestern Medical Center in Dallas, small molecule clinical trials like one involving glycerol phenylbutyrate can range from $25 million to $50 million.
Trials investigating gene therapies cost significantly more.
“You can imagine if you could enroll multiple disorders into a blanket protocol for one multi-site clinical trial at $50 million versus doing ten disorders with individual protocols at $50 million per individual protocol, the costs can climb quickly—especially in the case of gene therapy,” said Goodspeed.
Even if clinical trials were not cost-prohibitive, there remains the clinician factor. From a practical standpoint, many physicians already feel overwhelmed by the need to memorize ICD-10 codes. As Linzer stated during on March 9, 2023, during the ICD-10 Coordination & Maintenance Committee Meeting led by CMS, committing countless ICD-10 codes to memory for each rare disease may not be plausible.
“We’re very sympathetic to [the cause], but that’s not the issue,” he told the audience. “Our concern is the number of potential patients and developing unique codes for a tiny group of patients.”
Linzer went on to cite situations where proposals for larger populations were denied, as examples.
“If this proposal was to move forward, we certainly have already expressed our disagreement with the expansion to the sixth character on the ‘under the epilepsy [category]’ … but we do have concerns about unique codes for very small patient populations,” he said. “We understand it’s helpful in the research and clinical areas, but it’s just an issue of how many codes can there be?”
In a separate interview with Inside Precision Medicine, Linzer stated that creating additional codes can create problems in data tracking. Problems arise when the medical community uncovers additional information about a condition that leads to code expansion. Because the original intent of the code is to track morbidity and mortality, the code cannot be deleted.
Now approaching his seventh birthday, Maxwell Freed has already beat the odds that claim nearly one-third of children with a rare disease succumbing to their condition before their fifth birthday. Yet, the battle is far from over, as his mother, and countless other parents, continue advocating for their children in search of Federal support and cures.
“Mothers can pull from a source of energy that doesn’t exist,” Freed said of her ongoing efforts. “You hold your baby and know there’s nothing you wouldn’t give.”
As of press time, Freed’s applications for an ICD-10 assigned to SLC6A1 have remained unsuccessful and she received her most recent rejection in early 2024. Meanwhile, her son’s life—and those of others—hang in the balance.
Her solution? “I’ve learned how to fight like a mother.”
A mother’s enduring love is unmatched, and mothers never give up.
Read more:
- What We Do. The National Institutes of Health website. Accessed on February 25, 2024.
- The Promise of Precision Medicine: Rare Diseases. The National Institutes of Health website. Accessed on February 28, 2024
- Numbers: Rare Disease Facts. The Global Genes website. Accessed on February 28, 2024.
- Rare Disease: Although Limited, available Evidence Suggests Medical and Other Costs Can Be Substantial. The U.S. Government Accountability Office website. Accessed on February 28, 2024.
- Guha, M. Urea cycle disorder drug approved. Nat Biotechnol 31, 274 (2013).
- “The 10 Most Expensive Drugs on the Market.” The Talk to Mira website. Accessed on February 28, 2024.
- ICD-10 Coordination and Maintenance Committee. The Centers for Disease Control and Prevention website. Last reviewed October 17, 2022. Accessed on February 24, 2024.
- Kamada’s Prism Healthcare Map. Prism 2022.
- Kern SE. Challenges in conducting clinical trials in children: approaches for improving performance. Expert Rev Clin Pharmacol. 2009 Nov 1;2(6):609-617. doi: 10.1586/ecp.09.40. PMID: 20228942; PMCID: PMC2835973.
- Institute of Medicine (US) Committee on Clinical Research Involving Children; Field MJ, Behrman RE, editors. Ethical Conduct of Clinical Research Involving Children. Washington (DC): National Academies Press (US); 2004. 2, The Necessity and Challenges of Clinical Research Involving Children.
Frieda Wiley, PharmD, is an award-winning medical writer, best-selling author, speaker, and pharmacist who has written for O, Oprah Magazine, the National Institutes of Health, American History, Pfizer, Merck, AstraZeneca, and many more notable organizations.
The post Fight Like a Mother: When an ICD-10 Code Determines Life or Death appeared first on Inside Precision Medicine.
cdc disease control congress trump pandemic covid-19 treatment testing clinical trials therapy mortality europe world health organizationGovernment
No Fooling: Gov. Newsom’s $20 Minimum Wage Hits April 1
No Fooling: Gov. Newsom’s $20 Minimum Wage Hits April 1
Authored by John Seiler via The Epoch Times (emphasis ours),
A sign is posted on the…
Share this:


Authored by John Seiler via The Epoch Times (emphasis ours),
Commentary
I wish we could call “April fool!” on the $20 minimum wage hitting California fast-food restaurants on April 1. But the wage hike signed into law last September by Gov. Gavin Newsom is really going to hit hard.
Last December, Pizza Hut announced it would lay off more than 1,200 delivery drivers across the state. It switched to independent deliver services for home delivery. On March 25, the Wall Street Journal reported on driver Michael Ojeda, 29, “who previously supported his mother and partner on his Pizza Hut delivery wages.” He told the paper, “Pizza Hut was my career for nearly a decade and with little to no notice it was taken away.”
Round Table Pizza also laid off 73 drivers. And, “In San Jose, Brian Hom, owner of two Vitality Bowls restaurants, now runs his stores with two employees, versus four workers that he typically used in the past. That means it takes longer to make customers’ açaí bowls and other orders, and Hom said he is also raising prices by around 10 percent to help cover the increased labor costs. ”
Mr. Hom said, “I’m definitely not going to hire anymore.”
The $20 wage increase affects only chains with 60 or more restaurants nationwide. One effect might be to discourage national chains from setting up here. If a chain has, for example, 55 restaurants outside California, it would be hesitant to establish five restaurants in the Golden State because that would impact its wage structure everywhere else.
The $7.25 federal minimum wage applies in 20 states with no higher state wage. If a restaurant company operating in those states expanded to California, the disparity between $7.25 and $20 would be a shock to the company.
Another big effect will be on all other California businesses, not just restaurants with fewer than 60 operations nationwide. The state minimum wage overall went up fifty cents to $16 an hour on Jan. 1. The best workers at $16 will gravitate to the $20 jobs, effectively putting pressure on companies to pay more than $16. Companies that can’t do so will go out of business.

We won’t know for a couple of months, but California’s unemployment rate could go much higher. According to the U.S. Bureau of Labor Statistics, the state’s unemployment already has risen from 5.0 percent last September to 5.3 percent in February, the highest in the nation. The next highest is Nevada at 5.2 percent. Rival Texas is 3.9 percent and Florida is 3.1 percent.
Higher unemployment also will raise costs for the state’s troubled Employment Development Department. Due to incompetence by the Newsom administration, massive fraud during COVID-19 left the state $20 billion in debt to the federal government. Worse, reported California Globe on Feb. 29, higher interest rates from the Federal Reserve Board mean “the state can expect to have to make an interest only payment of about $500 million dollars instead of the $330 million that was planned for in Gov. Gavin Newsom’s budget for fiscal 2024-25,” which begins on July 1. It must be paid in September.
Newsom’s Political Future
Mr. Newsom can be a savvy politician. But he has a problem with economic realities. For eight years as lieutenant governor, he sat at the feet of Gov. Jerry Brown, who demonstrated how to prevent a budget from getting out of control. Instead, as governor Mr. Newsom went on spending sprees with the $97 billion surplus, everyone, including him, said couldn’t last. It didn’t.
Now he’s staring down a $38 billion budget deficit, according to his Jan. 10 budget proposal; or $73 billion, according to the Legislative Analyst’s latest projection.
The $20 minimum wage will kill many thousands of jobs, canceling the taxes of those workers while they are unemployed, while increasing unemployment costs. Albeit the $20 wage will bring in higher taxes from the workers still employed.
Employers, commonly in the upper middle-class, will suffer fewer profits, cutting into the income taxes they pay. Many even will call it quits and fold up their businesses, or move to more reasonable states.
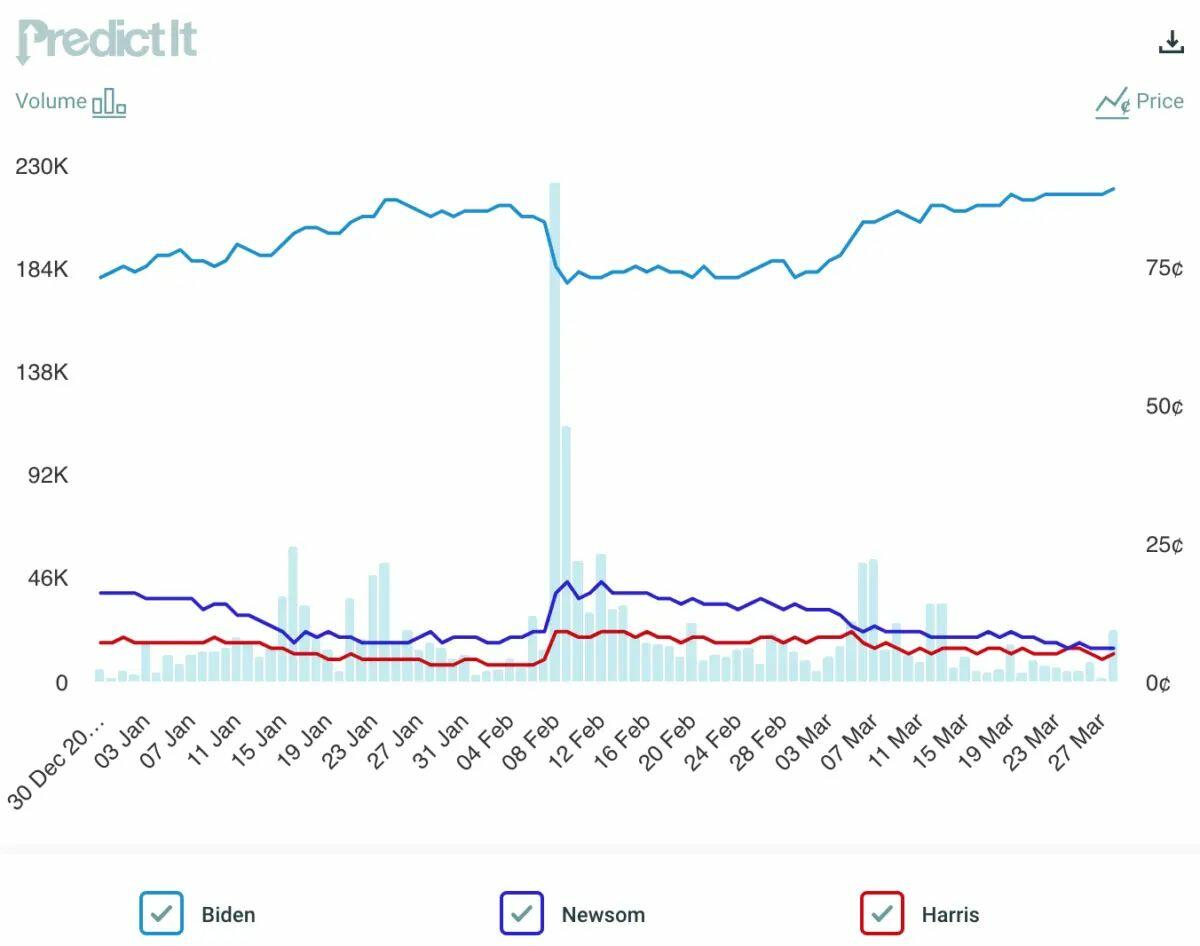
All this will hit this summer as Mr. Newsom’s presidential ambitions could still advance should President Joe Biden’s mental faculties decline much further. All that still is a long shot, of course. The PredictIt betting on Mr. Newsom gaining the nomination has been decreasing lately (middle line in the graph below), from 18 cents on Feb. 9 to 6 cents on March 29. Mr. Biden’s (top line) rose from 72 cents to 89 cents. Vice President Kamala Harris finished at 4 cents, below Mr. Newsom.
The point is it’s not impossible Mr. Newsom could get the nomination. If he does, California’s rising unemployment rate, the massive budget deficit, homelessness, high housing costs, and crime will be a target-rich environment for the Republicans’ presumptive nominee: former President Donald Trump.
Mr. Newsom could have avoided the unemployment crisis if he simply had pushed the $20 minimum wage into the future to 2027, when he will be out office. Then it would have been the next governor’s problem.
Conclusion: Expect More Joblessness
A higher minimum wage usually kills jobs, unless it is genuinely in line with an area’s cost of living. The current statewide $16 minimum wage is the second-highest of any state in the country, after Washington state’s $16.28. And Washington, D.C., not a state, is the highest at $17.00. All are areas with high expenses.
The biggest problem for California will be the $20 wage in rural areas. Although not as cheap to live in as Mississippi, it’s cheaper than living in San Francisco or Santa Monica. Which also means a lower minimum wage would be more sensible inland. Instead, the $20 wage will wipe out many more fast food jobs per capita inland than in the coastal areas.
The $20 wage is also going to increase prices for those still going to fast-food places. If inflation continues or gets worse, that will boost prices even more, leading to fewer customers, followed by even more layoffs.
Tinkering with the economy has consequences. Starting on April Fools’ Day, California will be finding out how an excessive minimum wage increase is one of the worst ones.
Views expressed in this article are opinions of the author and do not necessarily reflect the views of The Epoch Times or ZeroHedge.
International
Did The COVID Psyop Fail?
Did The COVID Psyop Fail?
Authored by Todd Hayen via Off-Guardian.org,
As you all know, I have not been one to believe that the tides are…
Share this:

Authored by Todd Hayen via Off-Guardian.org,
As you all know, I have not been one to believe that the tides are turning. But lots of people think they are. They cite many victories, in court, in the streets, with family and friends.
The fact that the agenda has not sent out a second wave of horror and fear propaganda is also rather telling to these folks. Where is the next pandemic? What happened to Covid’s diabolic never-ending run of mutations, what happened to Monkey Pox? What happened to Disease X?
Yes, all this could still happen, but it seems there have been more false starts—starts that didn’t go anywhere. But if so, you would think they wouldn’t have put them out there just to not have them continue. It’s been rather weird, like an electrical storm you see on the horizon with its threatening lightning strikes, but it never gets close enough to warrant closing the cellar door.
How about CBDCs? And the Digital IDs? You hear a lot about these, but nothing that is concretely happening to implement them. Is it happening in other places? Australia? Germany? The UK? Of course, a lot is said about it, on YouTube, and in alt media. Lots of talking heads, but how imminent is it? Actually, I won’t dwell on this, I have no doubt all of this is coming, but has the dragon been wounded? Even a little bit? Has this march into oblivion been slowed down?
Maybe there is no wounding of the general juggernaut of world rule by the schmucks who are claiming power. Although even that sacrosanct organization may have suffered from shell damage. Wasn’t DAVOS not all that they expected this past year? Hasn’t there been some pretty obvious whiplash from some leaders in their little club? How about the UN and the “sustainable development” circus? How is that going?
Anyway, I digress. Although the health of the world agenda, including all of these projects I mention, are all part of it, Covid, and pandemics in general, are the specific topics of this article.
I don’t buy any of this talk of victory for a New York minute. This is like cancer, you can’t claim victory until it is ALL gone, every last scrap of it. Remissions are nice, but if you’ve still got cancer in your body somewhere, it is only a time-out. I feel that this is similar. Even if one cell survived, it would start multiplying again and wouldn’t stop until it was big and gnarly and spitting out all the garbage this monster has been known to spit out. So, I don’t buy it…but…
Is it possible that at least one battle was won? Maybe, but just because they have pulled the troops back doesn’t mean they didn’t still take the city and got essentially what they stormed in for. I may still say that is a possibility. I mean, what did they want as a consequence of their Covid campaign? Did they want 100% compliance, with billions of sheep bowing down to them? Did they want everyone locked up in their own little cage, ala 1984, each of us in a squalid apartment with just a giant TV in the middle of it so Big Brother could blab at us all day long? If that is true, then indeed the psyop failed, because they didn’t get that—at least not yet.
But what if they got this: a toxic injection placed in billions of people worldwide that will kill untold millions over the course of about 20 years? Not only that, but the injection will render another untold millions sterile. Do the math here: how many people would need to be sterilized over 20 years to reduce the population worldwide by 1 billion? 2 billion? What other havoc could such a death jab wreak? What untold horrors are yet to overcome us? Your guess is as good as mine. Think zombies here, think soulless ghouls, think humans with no empathy, think lost humanity.
And that’s just the physical consequences. What about the psychological success they have had with the Covid campaign? Sure, many participants have shot them the bird regarding more boosters, and have ignored more threats of losing jobs over vaccine resistance. Sure, the courts have ruled in Canada that the illustrious leader here performed a no-no with his reckless enactment of the Emergency Act, and as a result, lawsuits are flowing into the courts. Does all this mean that no one fell for the psychological operation? That no one was mentally affected by the lockdowns, the masks, the closure of schools, churches, and other institutions? Does it mean that we have all recovered from the trauma of those three years, and mentally and emotionally we are just back to square one—all normal again?
If anyone reading this knows anything about hypnosis, they probably understand what hypnotic suggestion is all about. It is real, folks. What has been altered subliminally in our unconscious minds could be quite formidable. We are being programmed for better performance in future projects the agenda has in store for us. Most of the shrews reading this are safe from this brainwashing (hopefully) because we closed our eyes during the deadly meteor storm perpetrated by the fear-mongering agenda (watch The Day of the Triffids to understand that reference!) But those out there who got caught up in it and drank the delayed-reaction Kool-Aid—are all like sleeper spies from the Cold War, soon to be re-activated at some future date to continue complying with TPTB’s bidding.
Here I go again. I am supposed to be entertaining the possibility that the Covid psyop failed, not suggesting evidence to prove its great success. Sorry. Well, maybe it didn’t go as well as they wanted it to go. It does seem there was a lot more gas in the tank and that they could have pushed it a bit further than they did. They were doing pretty well, but they just fizzled out. Maybe they did expect more people to get vaxxed, maybe that was a disappointment. They sure looked like they were going for the whole enchilada with all their “you’ve GOT to get vaccinated!!” hoopla. Maybe they got too much pushback from us shrews. So many angry shrews showed up pretty quickly. And the shrews that were already on the scene, who were not surprised with all these shenanigans to begin with, just got louder and louder. Sure, not many sheep flipped, but some did. Their booster campaign is floundering (in my opinion, only because they turned the heat down, or off entirely).
So maybe they did get nicked a bit. Maybe a few arrows penetrated the armour, and they backed off a step or two. Maybe we did surprise the bastards with our resolve, tenacity, wit, and refusal to play the game.
But then again, maybe not.
Government
“The US Economy Is Inverted”: How The Flood Of Illegal Immigration Is Delaying The Official US Recession
"The US Economy Is Inverted": How The Flood Of Illegal Immigration Is Delaying The Official US Recession
By Dhaval Joshi, Chief Strategist…
Share this:

{kind=link}
{kind=link}
By Dhaval Joshi, Chief Strategist at BCA Research
Summary
-
The US economy is highly unusually ‘inverted’. The constraint on the economy is not labor demand, it is labor supply.
-
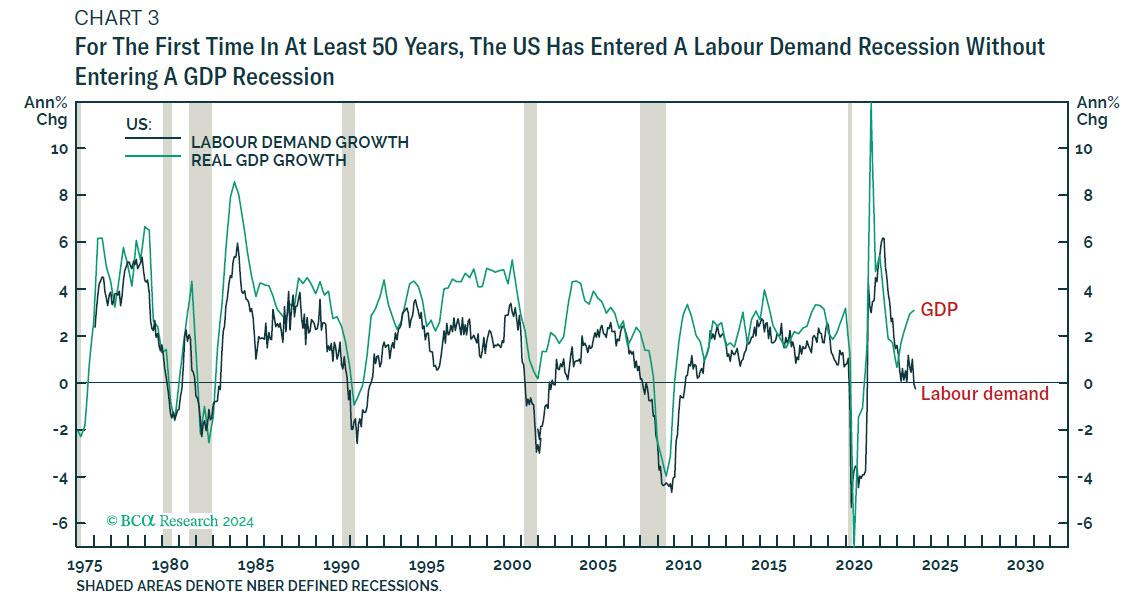
Hence, the US economy has highly unusually entered a labor demand recession without entering a GDP recession.
-
Nevertheless, for the stock market, a labour demand recession implies a profits headwind, because it is only when profits come under pressure that labour demand goes into recession.
-
Against this, wage disinflation would allow long-duration bond yields to fall, which would provide a countervailing valuation tailwind.
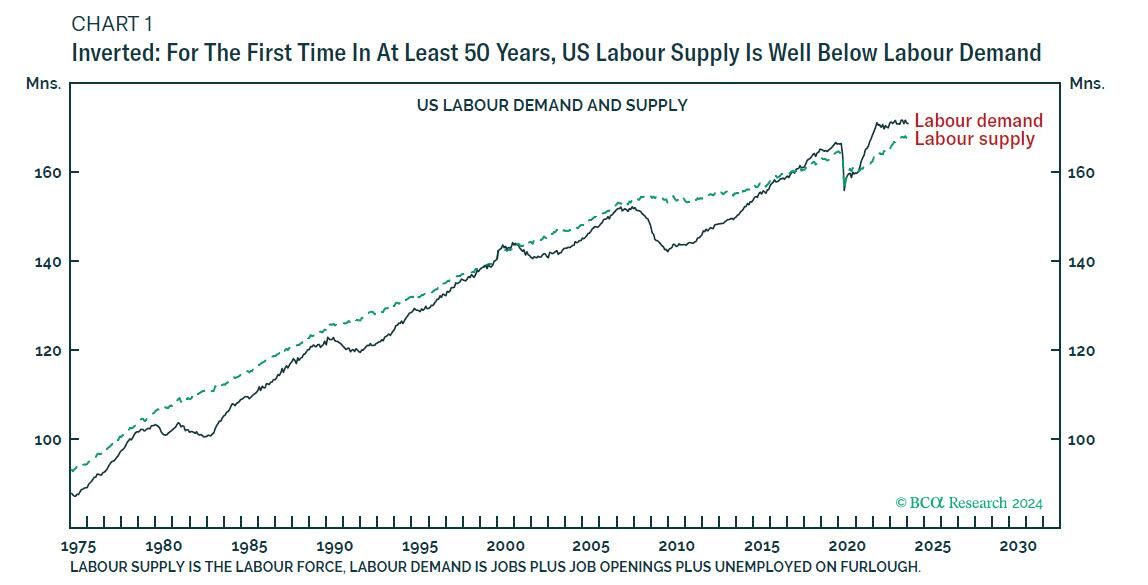
The pandemic might seem like a distant memory, but for the US economy the pandemic’s legacy is still the big story. For the first time in at least fifty years, US labor supply is running well below labor demand. The big story is that the US economy is ‘inverted.’
{kind=link}
Therefore, we must analyze the post-pandemic inverted economy very differently to the pre-pandemic economy. Normally, labor demand – being less than labor supply – is the constraint on economic output and thereby drives the cycle. But in an inverted economy, labor supply – being less than labor demand – is the constraint on output and thereby drives the cycle.
Before the pandemic, all downswings caused labor demand to fall well below labour supply. In the subsequent upswings, labor demand gradually caught up with supply…until the next downswing caused a fresh slump in labor demand. And the cycle repeated. Importantly though, all pre-pandemic cycles were driven by the demand side.
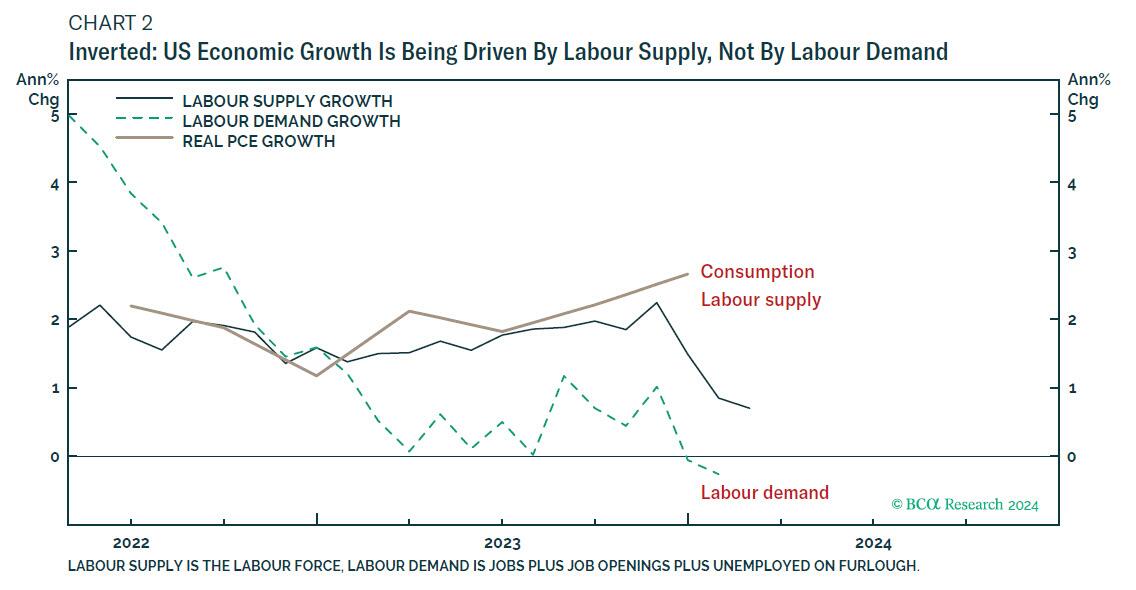
Then came the pandemic, and the longstanding pattern inverted. Labor supply suffered the more protracted slump, from which it has gradually caught up with labor demand. Meaning that in the last couple of years, the cycle is being driven not by what is happening to labor demand, but by what is happening to labor supply.
Interest rate hikes work by choking demand, which is exactly what has happened recently. US labor demand is tipping into recession. Jobs plus job openings today are less than they were a year ago. Whenever this happened pre-pandemic, the economy tipped into recession too. But for the first time in at least fifty years, the economy is entering a labor demand recession without entering a GDP recession.
This is because in an inverted economy the constraint on the economy is not labor demand, it is labor supply. Despite weaking
labor demand, labor supply has played catch up to demand and thereby driven economic growth.
As labor supply has caught up with labor demand, it has narrowed the gap between demand and supply. This has created the perfect macro backdrop of robust economic growth with wage disinflation, a Goldilocks setup for financial assets. The pressing question for the coming 6-12 months is, what happens next to labor supply, labor demand, and their interplay?
Why The US Economy Inverted
But first, let’s tackle the obvious question. Why is US labor supply running well below labor demand?
There are two reasons: after the pandemic, prime aged (25-54) workers left the labor force; and older aged (55+) workers retired early, generating millions of so-called ‘excess retirements.’
The economically inactive make no contribution to labor supply. Yet they still consume the goods and services that generate labor demand. This they do by using savings or, in the case of early retirees, by tapping into their retirement assets and income early. Thereby, the plunge in prime-aged labor participation combined with excess retirements caused labor supply to fall well below labor demand.
Subsequently, the plunge in prime-aged labour participation has fully reversed, causing labor supply to recover strongly. But the excess retirements have not reversed and are unlikely to reverse
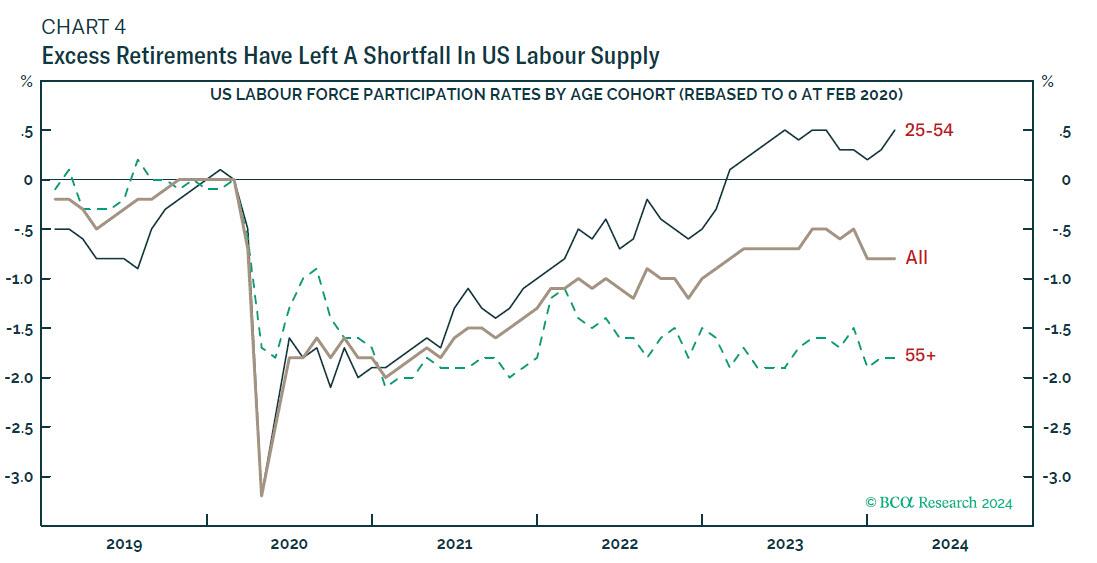
This means that the strong recovery in labor supply is now exhausted, with labor supply still several million people below labor demand. The economy is still inverted.
US Labour Demand Is Already In Recession, But GDP May Dodge The Bullet
To repeat, US labor demand has already tipped into recession. But in the inverted economy – where labor supply is the constraint on output – labor supply is driving the GDP cycle.
It follows that a GDP recession would require one of two things:
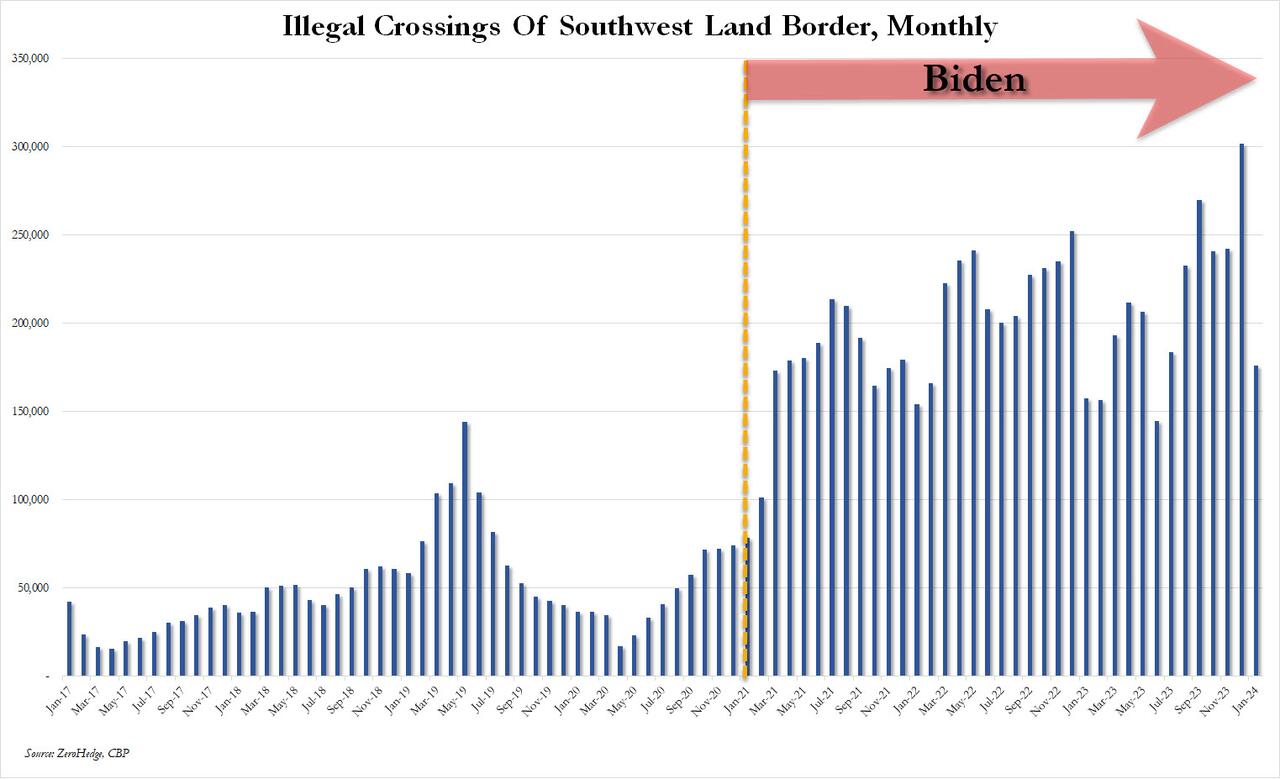
- Labor supply must outright contract. However, with the recent surge in illegal migration – most of which does eventually get counted in the survey-calculated labor supply – a sustained contraction in labor supply seems unlikely. Of course, this could change under a new Trump administration, or...
- Labor demand must contract so sharply – by about 3.5 million jobs – that the economy would ‘un-invert’. Once un-inverted, contracting labor demand would once again drive GDP into recession, as in all pre-pandemic cycles.
But if labor demand contracts more gently – as now – then the US economy could experience a sustained labor demand recession without a GDP recession, making it difficult for the National Bureau of Economic Research (NBER) to designate it an official recession.
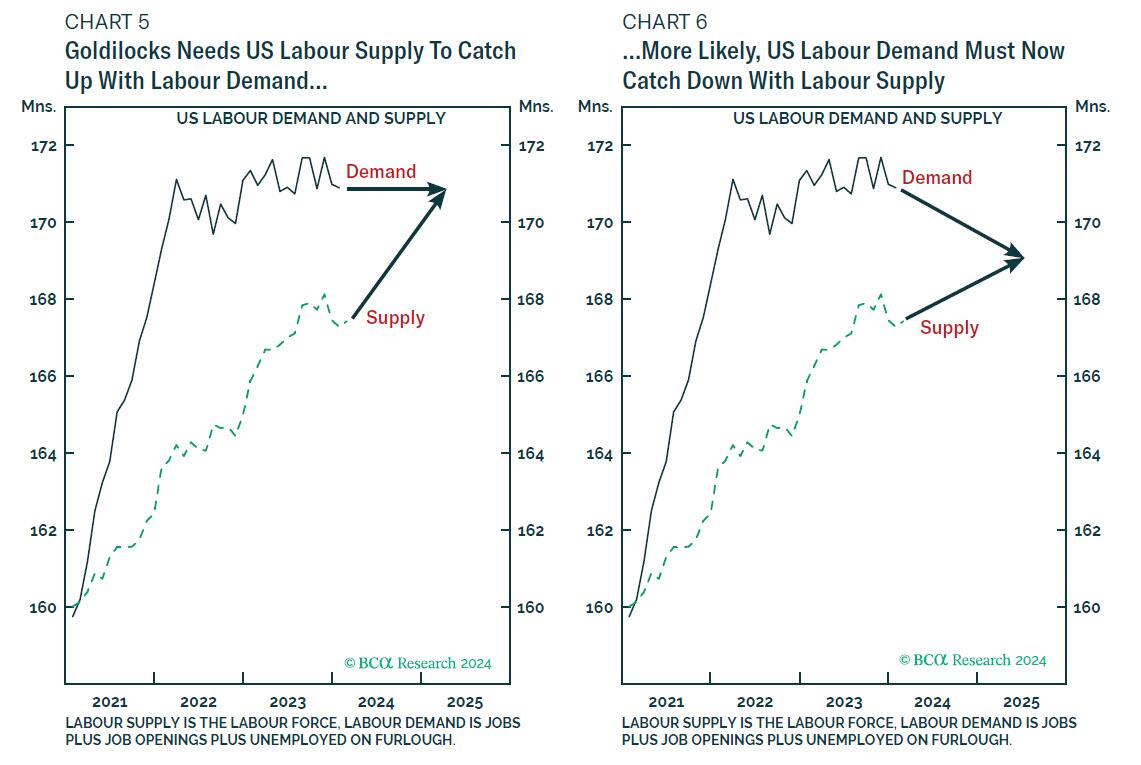
This ‘halfway house’ in which GDP is not in recession, but labor demand is in recession and gently ‘catching down’ with labor supply is a distinct possibility – because it is the least painful way for the Federal Reserve to steer wage inflation back down to the 3 percent rate that is needed for price inflation to stabilise at 2 percent (Chart 5 and Chart 6).
Yet though the economy could dodge the ‘NBER official recession’ bullet, a labor demand recession combined with stagnant per capita real incomes would very much feel like a recession.
For the stock market, a labor demand recession implies lower profits because it is only when profits come under pressure that labor demand goes into recession. Against this, wage disinflation would allow long-duration bond yields to fall, which would provide some countervailing support to stock valuations. In combination this would imply the stock market was rangebound while high-quality bonds rallied.
But there is another factor to consider. The euphoric pricing of anything AI-related is a separate and independent risk to the stock market. Absent this risk the macro backdrop would imply a neutral allocation to stocks versus cash. But this additional risk ratchets down my 6-12-month allocation to mildly underweight.
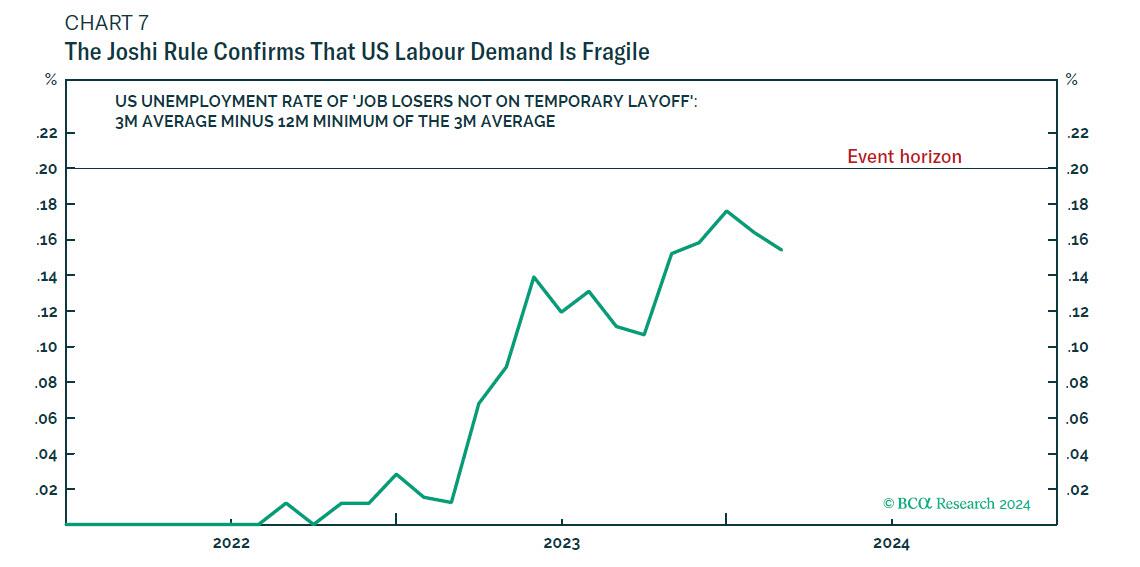
For those who can time this, go underweight stocks when the ‘Joshi rule’ is triggered. Or, when the rally reaches a collapsed complexity that presages an imminent reversal.
More in the full note available to pro subscribers.


The Era Of Informed Consent Is Over


Southwest Airlines challenged on its low-cost claims

My Weekly Reading for March 31, 2024


“The US Economy Is Inverted”: How The Flood Of Illegal Immigration Is Delaying The Official US Recession


Why The Department Of Justice Wants To Take Down Apple


Remote customer service jobs: What they pay & how to get one


Pandemic Whiskey Boom Turns To Hangover


Did The COVID Psyop Fail?


Big shipping company files for Chapter 11 bankruptcy


How Much Do Food Stamps, Social Security, And Medicare Support The Economy?
-

 Spread & Containment3 weeks ago
Spread & Containment3 weeks agoIFM’s Hat Trick and Reflections On Option-To-Buy M&A
-

 International1 week ago
International1 week agoParexel CEO to retire; CAR-T maker AffyImmune promotes business leader to chief executive
-

 International3 weeks ago
International3 weeks agoEyePoint poaches medical chief from Apellis; Sandoz CFO, longtime BioNTech exec to retire
-

 International3 weeks ago
International3 weeks agoWalmart launches clever answer to Target’s new membership program
-

 Uncategorized1 month ago
Uncategorized1 month agoKey Events This Week: All Eyes On Core PCE Amid Deluge Of Fed Speakers
-

 Uncategorized4 weeks ago
Uncategorized4 weeks agoEvidence And Insights About Gold’s Long-Term Uptrend
-

 Uncategorized1 month ago
Uncategorized1 month agoA Global, Digital Coup d’État
-

 International1 week ago
International1 week agoJapanese Preprint Calls For mRNA VaccinesTo Be Suspended Over Blood Bank Contamination Concerns