International
Cyclical Rally Could Look Very Different From Here
Cyclical Rally Could Look Very Different From Here
By Michael Msika, Bloomberg Markets Live reporter and strategist
A months-long rally in…
Share this:


By Michael Msika, Bloomberg Markets Live reporter and strategist
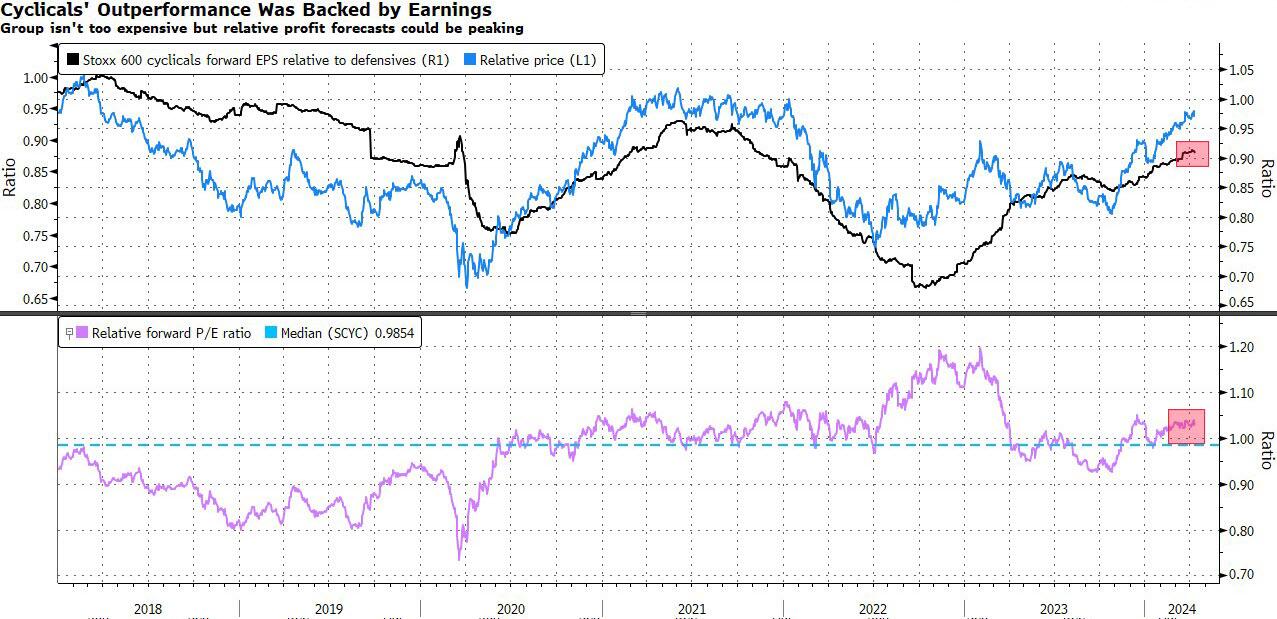
A months-long rally in European cyclicals has left some stocks looking outright expensive, raising risks for them as the earnings season is about to start.
Cyclical sectors such as autos, industrials and financials have beaten the overall market hands down so far this year, with a 9% gain. Since the end of October, the Stoxx 600 Cyclical index has added 26%, beating defensive sectors by nearly 20 percentage points. That’s put them into the danger zone for profit-taking, amid signs the group is hitting overbought levels.
JPMorgan strategist Mislav Matejka notes cyclicals have in fact outperformed defensives for 18 months and trade at a significant premium. Other than energy, which he sees as a good hedge against elevated geopolitical risk, Matejka is neutral or bearish on most cyclical shares. “Defensives could look better from here, especially if the overall market starts to weaken, and if earnings growth acceleration expectations do not materialize,” he says.
Not all cyclicals are in the same boat, though. Gains on energy and mining shares follow a long period of underperformance and are driven by geopolitics as well as a brightening world economy. Nor do share valuations seem excessive for commodities and banking shares.
This segment of cyclicals is likely to outperform, according to Goldman Sachs strategists Peter Oppenheimer and Sharon Bell. They recently upgraded banks and energy to overweight and miners to neutral. However, they cut their view on industrials, citing expensive valuations.
Trading at nearly 20 times forward earnings — a 40% premium to the broader market and in the 90th percentile relative to their history — European industrials do look pricey. They also appear to have seriously overshot the recovery in PMIs — the last time the sector traded at such levels was just after the pandemic when European manufacturing was expanding rapidly. The fear is that companies pricing so much good news risk punishment if they disappoint in the upcoming earnings season.
Bank of America strategists are among those sticking to a very cautious stance. Wary of recent winners such as capital goods, BofA’s Sebastian Raedler sees scope for rotation into beaten-down defensives such as as food and beverages, though he remains overweight miners and chemicals. “Cyclicals overall are priced for sharp EPS upgrades,” he adds.

Cyclicals still have their fans, who point out the recent outperformance was driven by improved earnings estimates and that the overall group only trades at slightly above-average valuations compared with defensives. With interest-rate cuts due to kick off in the coming months, cyclical shares could enjoy further gains, many strategists, including at Barclays and Natixis, expect.
“Don’t fight the soft-landing narrative,” say Natixis strategists Florent Pochon and Emilie Tetard. They like European cyclicals tactically, in anticipation of a pick-up in European and Chinese economic growth, and the first European Central Bank rate cut in June.
Spread & Containment
Stuck On Failure At The WHO
Stuck On Failure At The WHO
Authored by Kevin Roberts and Robert Redfield via The Epoch Times (emphasis ours),
Four years have passed since…
Share this:


Authored by Kevin Roberts and Robert Redfield via The Epoch Times (emphasis ours),
Four years have passed since the onset of COVID-19 and the global mishandling of its spread. Now, the same governments and international organizations that lied about the last pandemic are negotiating a new pandemic agreement and amendments to the International Health Regulations (IHR) at the World Health Organization (WHO).
The main culprit hasn’t changed. Although the Chinese Communist Party (CCP) has never been held accountable for its complete refusal to adhere to previous IHR agreements or its ongoing obstruction of a thorough investigation into the virus’s origins, Beijing is now collaborating with the Biden administration on this new accord.
So naturally, the new agreement advances China’s interests. Successive drafts focus on everything, from sending taxpayer dollars overseas to weakening intellectual property rights and empowering the WHO over the national sovereignty of the United States. Yes, that’s the same WHO that failed to insert a team of global experts in the first few weeks of the COVID-19 outbreak in China (as required by IHR), instead capitulating to the CCP and allowing it to define the international response.
The latest version of the agreement even mandates that parties provide financial and technical assistance to developing countries. Of course, the United States has a long, robust history of providing such assistance—President George W. Bush’s President’s Emergency Plan for AIDS Relief (PEPFAR) is one good example—but such assistance has always been voluntary, not obligatory.
Unsurprisingly, China stands to benefit from these provisions intended to help “poor” countries. Despite having the second-largest economy in the world, the United Nations considers China to be a “developing country.” That’s right. The country that started the COVID-19 pandemic will not only suffer zero consequences for its actions but, should the United States sign this agreement, stand to benefit from mandatory transfers of funds from U.S. taxpayers.
China would also benefit from other provisions in the agreement that push governments to promote “sustainable and geographically diversified production” of pandemic-related products (like vaccines), invest in developing country capacity and access to proprietary research, use the “flexibilities” of the Agreement on Trade-Related Aspects of Intellectual Property Rights to override patents, and encourage rights holders to forego or reduce royalties and consider time-bound waivers of intellectual property rights.
China, notorious for its theft of intellectual property, would be sure to exploit this privilege.
All this would severely curtail future investment in health research—exactly the opposite incentive that should be applied if we are to be prepared for a future pandemic. And to make matters worse, the agreement almost entirely ignores addressing the countless shortcomings of current international processes in responding to pandemics, such as obligating governments to grant immediate access to international health expert teams to assess the threat of suspected outbreaks and to provide full and timely disclosure of genomic data.
Of course, overseeing sustainable and geographically diversified production, massive transfers, and distribution of up to 20 percent of diagnostics, therapeutics, or vaccines during a pandemic comes with a hefty price tag. The exact amount is not specified, but it is sure to include several commas.
In addition, the agreement would take a sledgehammer to American First Amendment free speech rights. The willingness of governments to use the pandemic to clamp down on unpopular ideas and opinions to “protect” public health and safety has proven durable. And this new agreement instructs governments to “cooperate, in accordance with national law, in preventing misinformation and disinformation.” China and Russia need no encouragement to censor speech. However, such language in an international agreement will encourage those in free countries who similarly wish to suppress unpopular opinions under the guise of countering misinformation and disinformation.
Indeed, the WHO itself seems offended by criticism. Earlier this year, Director-General Tedros Adhanom Ghebreyesus said that negotiations were occurring in a very difficult environment, facing a “torrent of fake news, lies, and conspiracy theories.” Ironically, this argument was the same one used against conservatives who subscribed to the increasingly credible lab leak theory.
In short, the new pandemic agreement should alarm all Americans. It is far more focused on redistributing income, transferring technology, and weakening intellectual property than on preventing, detecting, and responding to pandemics in the first place. It failed to address the elephant in the room—the total lack of enforcement in the IHR—and as written, it is nothing short of a power grab by the CCP-controlled WHO.
Our government must wholly reject it.
Views expressed in this article are opinions of the author and do not necessarily reflect the views of The Epoch Times or ZeroHedge.
International
Immigration And Its Impact On Employment
Is immigration why employment reports from the Bureau of Labor Statistics (BLS) continue defying mainstream economists’ estimates? Many are asking this…
Share this:

Is immigration why employment reports from the Bureau of Labor Statistics (BLS) continue defying mainstream economists’ estimates? Many are asking this question as the U.S. experiences a flood of immigrants across the southern border. Concurrently, many young college graduates continue to complain about the inability to receive a job offer. As noted recently by CNBC:
The job market looks solid on paper. According to government data, U.S. employers added 2.7 million people to their payrolls in 2023. Unemployment hit a 54-year low of 3.4% in January 2023 and ticked up just slightly to 3.7% by December.
But active job seekers say the labor market feels more difficult than ever. A 2023 survey from staffing agency Insight Global found that recently unemployed full-time workers had applied to an average of 30 jobs only to receive an average of four callbacks or responses.”
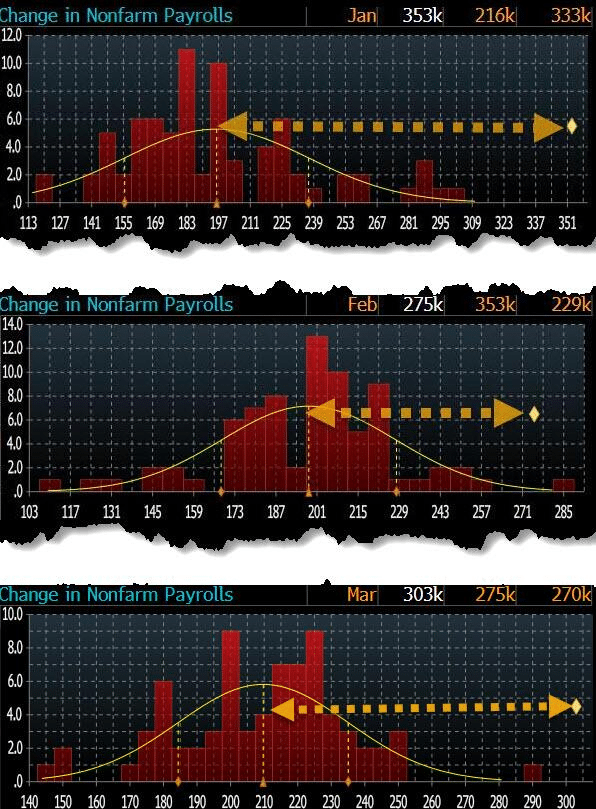
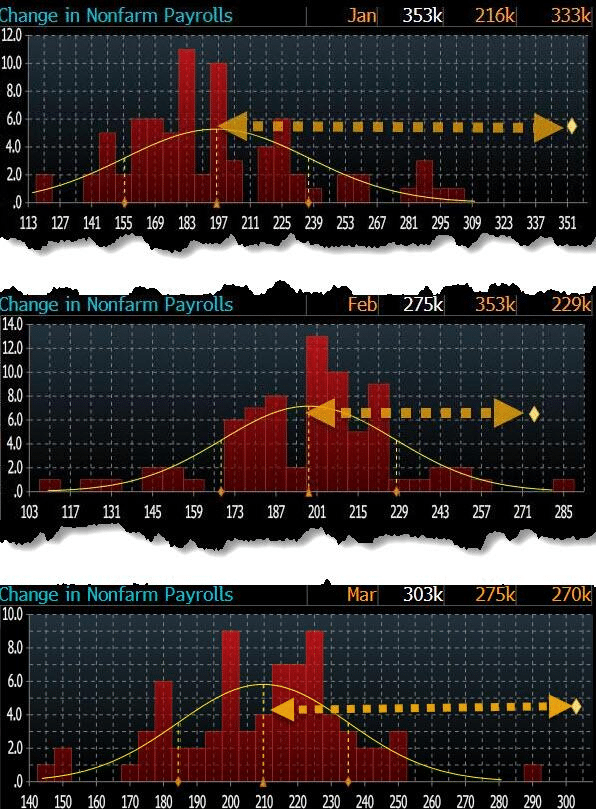
These stories are not unique. If you Google “Can’t find a job,” you will get many article links. Yet employment reports have been exceedingly strong for the past several months. In March, the U.S. economy added 303,000 jobs, exceeding every economist’s estimate by four standard deviations. In terms of statistics, a single four-standard deviation event should be rare. Three months in a row is a near statistical impossibility.
Despite weakness in manufacturing and services, with many companies recently announcing layoffs, we have near-record-low jobless claims and employment. According to official government data, the economy has rarely been more robust.

Such a situation begs an obvious question: How are college graduates struggling to find employment while the labor market remains so strong?
We may find the answer in immigration.
Immigrations Impact By The Numbers
A recent study by Wendy Edelberg and Tara Watson at the Brookings Institution found that illegal immigrants in the country helped boost the labor market, steering the economy from a downturn. Data from the Congressional Budget Office shows a massive uptick of 2.4 million “other immigrants” who don’t fall into the category of lawful immigrants or those on temporary visas. The chart below shows how this figure has spiked from a level of less than 500,000 at the beginning of the 2020s.

The most significant change relative to the past stems from CBO’s other non-immigrant category, which includes immigrants with a nonlegal or pending status.
“We indicate our estimates of ‘likely stayers’ by diamonds in Figure 2. In FY 2023, almost a million people encountered at the border were given a ‘notice to appear,’ meaning they have permission to petition a court for asylum or other immigration relief. Most of these individuals are waiting in the U.S. for the asylum court queue, which has over a million case backlog. In addition, over 800,000 have been granted humanitarian parole (mostly immigrants from Ukraine, Haiti, Cuba, Nicaragua, and Venezuela). These 1.8 million ‘likely stayers’ in FY 2023 may or may not remain in the U.S. permanently, but most are currently living in the U.S. and participating in the economy. CBO estimates that there were 2 million such entries over the calendar year 2023, which is consistent with higher encounters at the end of the calendar year.”

According to the CBO’s estimates for 2023, the categories of lawful permanent resident migration, INA non-immigrant, and other non-immigrant equated to 3.3 million net entries. However, the number is likely much higher than estimates, subject to uncertainty about unencountered border crossings, visa overstays, and “got-aways.”
As such, this influx of immigrants has significantly added to payroll growth and has accounted for the uptick in economic growth starting in 2022. While the uptick in border encounters began in earnest in 2021, as the current Administration repealed previous border security actions, there is a “lag effect” of immigration on economic growth.

However, not all jobs are created equal.
Immigration’s Impact On Job Availability
Since 1980, the U.S. economy has shifted from a manufacturing-based economy to a service-oriented one. The reason is that the “cost of labor” in the U.S. to manufacture goods is too high. Domestic workers want high wages, benefits, paid vacations, personal time off, etc. On top of that are the numerous regulations on businesses from OSHA to Sarbanes-Oxley, FDA, EPA, and many others. All those additional costs are a factor in producing goods or services. Therefore, corporations must offshore production to countries with lower labor costs and higher production rates to manufacture goods competitively.
In other words, for U.S. consumers to “afford” the latest flat-screen television, iPhone, or computer, manufacturers must “export” inflation (the cost of labor and production) to import “deflation” (cheaper goods.) There is no better example of this than a previous interview with Greg Hays of Carrier Industries. Following the 2016 election, President Trump pushed for reshoring U.S. manufacturing. Carrier Industries was one of the first to respond. Mr. Hays discussed the reasoning for moving a plant from Mexico to Indiana.
“So what’s good about Mexico? We have a very talented workforce in Mexico. Wages are obviously significantly lower. About 80% lower on average. But absenteeism runs about 1%. Turnover runs about 2%. Very, very dedicated workforce. Which is much higher versus America. And I think that’s just part of these — the jobs, again, are not jobs on an assembly line that [Americans] really find all that attractive over the long term.“
The need to lower costs by finding cheaper and plentiful sources of labor continues. While employment continues to increase, the bulk of the jobs created are in areas with lower wages and skill requirements.

As noted by CNBC:
“The continued rebound of these jobs, along with strong months for sectors like construction, could be a sign that immigration is helping the labor market grow without putting too much upward pressure on wages.”
This is a crucial point. If there is strong employment growth, wages should increase commensurately as the demand for labor increases. However, that isn’t happening, as the cost of labor is suppressed by hiring workers willing to work for less compensation. In other words, the increase in illegal immigrants is lowering the “average” wage for Americans.

Nonetheless, in the last year, 50% of the labor force growth came from net immigration. The U.S. added 5.2 million jobs last year, which boosted economic growth without sparking inflationary pressures.
While immigration has positively impacted economic growth and disinflation, this story has a dark side.
The Profit Motive
In a previous article, I discussed an interview by Fed Chair Jerome Powell discussing immigration during a 60-Minutes Interview. To wit:
“SCOTT PELLEY: Why was immigration important?
FED CHAIR POWELL: Because, you know, immigrants come in, and they tend to work at a rate that is at or above that for non-immigrants. Immigrants who come to the country tend to be in the workforce at a slightly higher level than native Americans. But that’s primarily because of the age difference. They tend to skew younger.“
You should read that comment again carefully. As noted by Greg Hayes, immigrants tend to work harder and for less compensation than non-immigrants. That suppression of wages and increased productivity, which reduces the amount of required labor, boosts corporate profitability.

The move to hire cheaper labor should be unsurprising. Following the pandemic-related shutdown, corporations faced multiple threats to profitability from supply constraints, a shift to increased services, and a lack of labor. At the same time, mass immigration (both legal and illegal) provided a workforce willing to fill lower-wage paying jobs and work regardless of the shutdown. Since 2019, the cumulative employment change has favored foreign-born workers, who have gained almost 2.5 million jobs, while native-born workers have lost 1.3 million. Unsurprisingly, foreign-born workers also lost far fewer jobs during the pandemic shutdown.

Given that the bulk of employment continues to be in lower-wage paying service jobs (i.e., restaurants, retail, leisure, and hospitality) such is why part-time jobs have dominated full-time in recent reports. Since last year, part-time jobs have risen by 1.8 million while full-time employment has declined by 1.35 million.

Not dismissing the implications of the shift to part-time employment is crucial.
Personal consumption, what you and I spend daily, drives nearly 70% of economic growth in the U.S. Therefore, Americans require full-time employment to consume at an economically sustainable rate. Full-time jobs provide higher wages, benefits, and health insurance to support a family, whereas part-time jobs do not.
Notably, given the surge in immigration into the U.S. over the last few years, the all-important ratio of full-time employees relative to the population has dropped sharply. As noted, given that full-time employment provides the resources for excess consumption, that ratio should increase for the economy to continue growing strongly.

However, the reality is that the full-time employment rate is falling sharply. Historically, when the annual rate of change in full-time employment dropped below zero, the economy entered a recession.

While there is much debate over immigration, most of the arguments do not differentiate between legal and illegal immigration. There are certainly arguments that can be made on both sides. However, what is less debatable is the impact that immigration is having on employment and wages. Of course, as native-born workers continue to demand higher wages, benefits, and other tax-funded support, those costs must be passed on by the companies creating those products and services. At the same time, consumers are demanding lower prices.
That imbalance between input costs and selling price drives companies to aggressively seek options to reduce the highest cost to any business – labor.
Such is why full-time employment has declined since 2000 despite the surge in the Internet economy, robotics, and artificial intelligence. It is also why wage growth fails to grow fast enough to sustain the cost of living for the average American. These technological developments increased employee productivity, reducing the need for additional labor.
Unfortunately, college graduates expecting high-paying jobs will likely continue to find it increasingly frustrating. Such is particularly the case as “Artificial Intelligence” gains traction and displaces “white collar” work, further squeezing the demand for “native-born” workers.
The post Immigration And Its Impact On Employment appeared first on RIA.
recession unemployment pandemic economic growth fed trump fda suppression unemployment mexico ukraineGovernment
How Ivermectin Trials Were Designed To Fail
How Ivermectin Trials Were Designed To Fail
Authored by Yuhong Dong via The Epoch Times (emphasis ours),
The use of ivermectin to treat COVID-19…
Share this:

{kind=link}
{kind=link}
{kind=link}

Authored by Yuhong Dong via The Epoch Times (emphasis ours),
The use of ivermectin to treat COVID-19 is an ongoing debate. The central conflict is that while many doctors have reported success in using ivermectin, some studies published in major journals suggest it is in fact ineffective.
{kind=link}
Even as the FDA recently has been removing misinformation it posted about ivermectin, the agency has maintained its original position regarding its effectiveness, namely that there isn’t evidence.
People who trust ivermectin claim the studies showing ineffectiveness are fraudulent, while people who are skeptical of its use for treating COVID-19 view it as an anti-science conspiracy theory.
As a professional with decades of research experience conducting dozens of clinical trials on antiviral drugs, I decided to dive deep into the studies purporting ivermectin’s ineffectiveness. What I found shocked me.
Legacy Media Report Ineffectiveness
Numerous preclinical studies have found that ivermectin has a broad range of effects on COVID-19, spanning from its initial impact on viral infection to the pathological changes the virus causes in our bodies.
Ivermectin inhibits the entire life cycle of SARS-CoV-2 in our cells from attachment, spreading, and replication (1, 2, 3).
Moreover, ivermectin is anti-inflammatory and organ-protective, which can potentially protect against severe COVID-related lung damage and acute respiratory distress syndrome, heart-related complications, and blood clots.
Ivermectin exceeds the approved antiviral effects of other medications, including Paxlovid, molnupiravir and remdesivir, which only target the virus and lack anti-inflammatory and organ-protective effects. Monoclonal antibodies have to be constructed specific to each variant and are very expensive.
In the pharmaceutical industry, clinical trials are commonly used to evaluate the efficacy and safety of drugs once their mechanism is demonstrated. There are two types of clinical trials: observational and interventional.
Observational studies are often conducted by doctors in clinical, hospital, or community settings to analyze the effects of drugs. The data is collected as observed in clinical practice with minimal interference.
Many doctors have observed the positive effects of ivermectin on their patients. An observational study conducted in Brazil with over 88,000 patients showed that ivermectin reduced the rates of infection, mortality, and hospitalization by 49 percent, 92 percent, and 100 percent, respectively, compared to nonusers.
Pharmaceutical companies are required to conduct interventional studies that meet the approval standards set by the U.S. Food and Drug Administration (FDA). Randomized clinical trials (RCTs) are frequently utilized to fulfill these requirements. This type of study is considered the gold standard and involves randomly assigning one group of patients to receive a specific drug while the other group does not receive it, then comparing the outcomes.
Legally and medically, ivermectin can be prescribed off-label to treat COVID-19 since it has already been approved by the FDA for other diseases.
Although many doctors have observed the positive effects of ivermectin in treating their patients, the media has specifically highlighted data from a few selected RCTs that have concluded it is ineffective in treating COVID-19.
However, some critical aspects were overlooked in those RCTs.
Improper Dosing
A drug’s therapeutic effects can only be observed when it reaches the appropriate concentration in the body and remains there for a few days, allowing sufficient time to work.
Improper dosing was a major issue in the RCTs that found ivermectin ineffective.
Recommended Dosage
According to Merck’s package insert for ivermectin (brand name Stromectol), a single oral dose of 0.2 mg/kg was officially recommended for treating parasitic diseases. There is no official dose for COVID-19.
The recommended dosage of ivermectin for treating COVID-19 is based on the clinical experiences of physicians worldwide.
The Front Line COVID-19 Critical Care Alliance (FLCCC) guidelines recommend taking 0.4 mg/kg of ivermectin daily, immediately after exposure. Once a cumulative dose in excess of 200 mg is reached, the risk of acquiring COVID-19 has been shown to be nearly zero.
It is common for a drug with multiple indications to have different doses for different diseases.
Moreover, ivermectin should be given with food, as it has a 2.6-fold higher bioavailability when taken with food rather than on an empty stomach. The Merck package insert (revised May 2022) also supports this and states: “Administration of 30 mg ivermectin following a high-fat meal resulted in an approximate 2.5-fold increase in bioavailability relative to administration of 30 mg ivermectin in the fasted state.”
FLCCC guidelines also recommend taking ivermectin “with or just following a meal for greater absorption.”
Yet this important dosing information is not reflected in the commonly used drug prescribing resource known as the Prescribers’ Digital Reference or PDR which states: “Take the number of tablets your doctor has prescribed all at the same time with water on an empty stomach. Do not eat any food within two hours before or after taking the tablets.”
So if a person takes the dose while fasting, they are getting only 40 percent of the recommended dose. For patients with a higher body weight, the effects of underdosing could be even more significant.
RCT Studies Used Inappropriate Dosing
In the most recent PRINCIPLE trial published in March, ivermectin was used at 0.3 mg/kg for only three days. Moreover, it was designed to dose the ivermectin without food: “Participants were advised not to eat two hours before or after taking ivermectin.”
In another RCT ACTIV-6 published in JAMA in October 2022, ivermectin was dosed in a fasting status, as the protocol stated: “Ivermectin should be taken on an empty stomach with water (30 minutes before a meal or 2 hours after a meal).”
Ivermectin was reported as dosed at 0.4 mg/kg for three days—a much shorter time period than it should be. However, in the protocol Table 4 in Appendix 16.3.3, the precise dosing was as low as 0.269 mg/kg, and 0.4 mg/kg is actually only the upper dose limit—not the real dose.
According to the worldwide recognized study guideline ICH Good Clinical Practice, clinical trials must adhere to ethical principles. Failure to do so would be considered study misconduct or fraud and would violate the principle of integrity.
Another JAMA study published in March 2021 repeated the same mistake in mild COVID-19 patients by suggesting they take 0.3 mg/kg for five days on an empty stomach.
An RCT study known as TOGETHER, published in March 2022 in the New England Journal of Medicine, underdosed ivermectin with 0.4 mg/kg for only three days and did not mention dosing with food.
Nevertheless, even at this low dose, the ivermectin still reduced hospitalization rates, death, and the need for mechanical ventilation compared to a placebo.
Clinical Improvement Despite Underdosing
It is inappropriate to conclude that ivermectin was ineffective based on these RCT studies with major design flaws.
Despite the poor study design, ivermectin showed clinical benefits and saved lives.
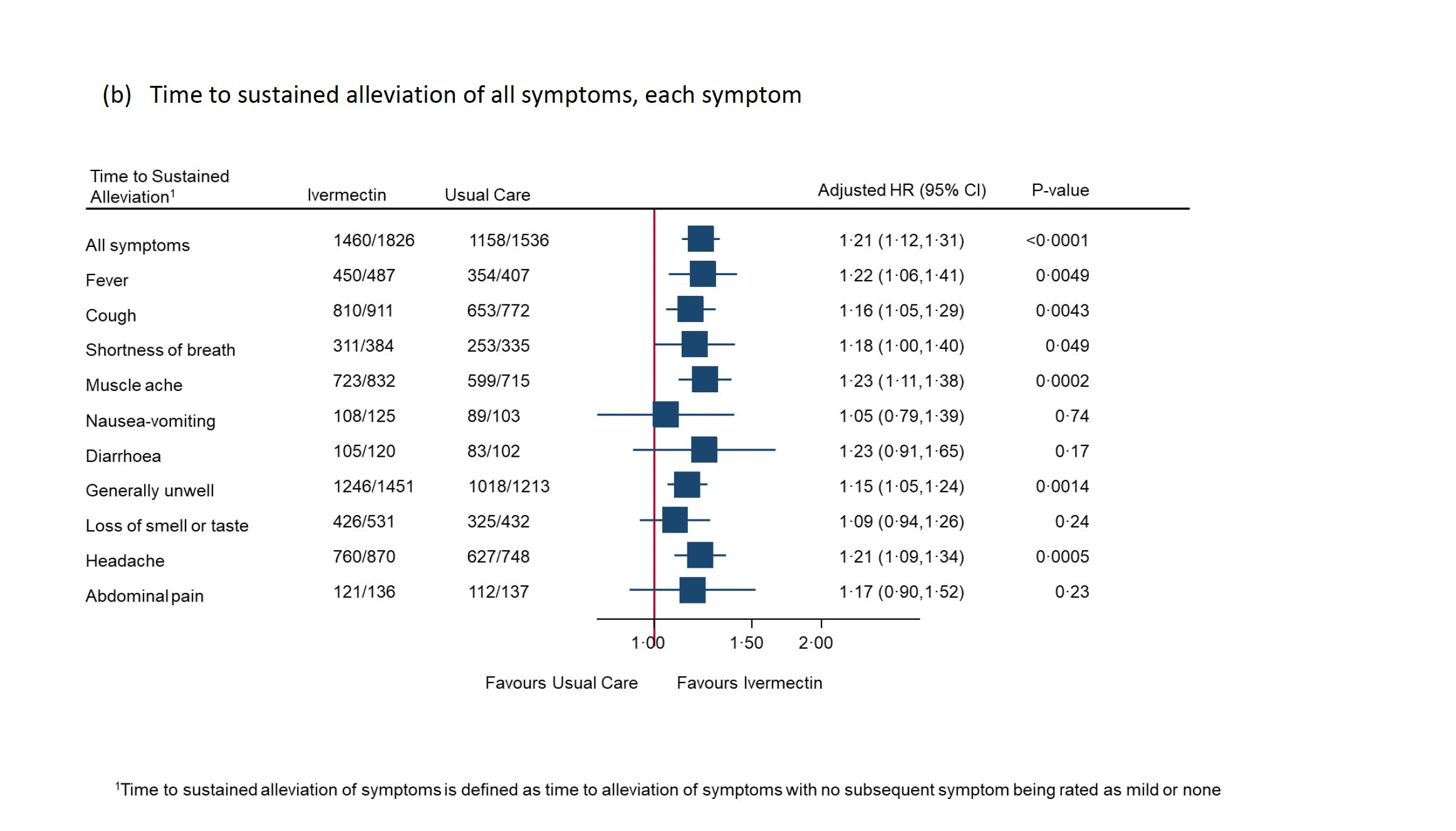
In the PRINCIPLE study, self-reported recovery was shorter in the ivermectin group than usual care, with a median decrease of 2.06 days. The statistical analysis showed that it met the predefined superiority criteria.
Furthermore, the analysis showed that ivermectin effectively reduced COVID-19-related hospitalizations and deaths. Only 1.6 percent of 2,157 patients in the ivermectin group experienced hospitalizations or deaths, compared to 4.4 percent of 3,256 patients in the usual care group.
Even a low dose of ivermectin has demonstrated the potential to save lives. However, the authors concluded, “Ivermectin for COVID-19 is unlikely to provide clinically meaningful improvement in recovery, hospital admissions, or longer-term outcomes.”
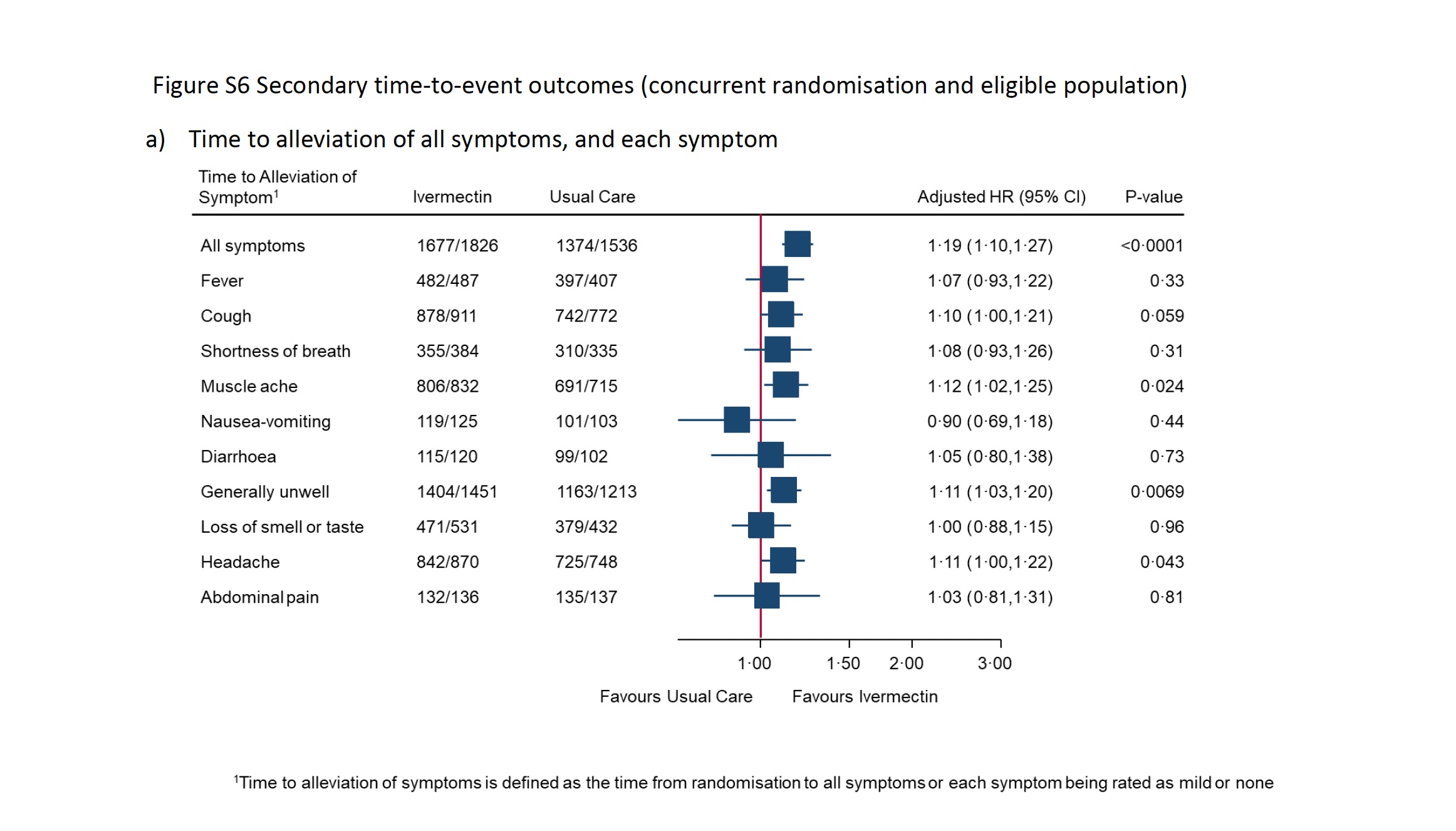
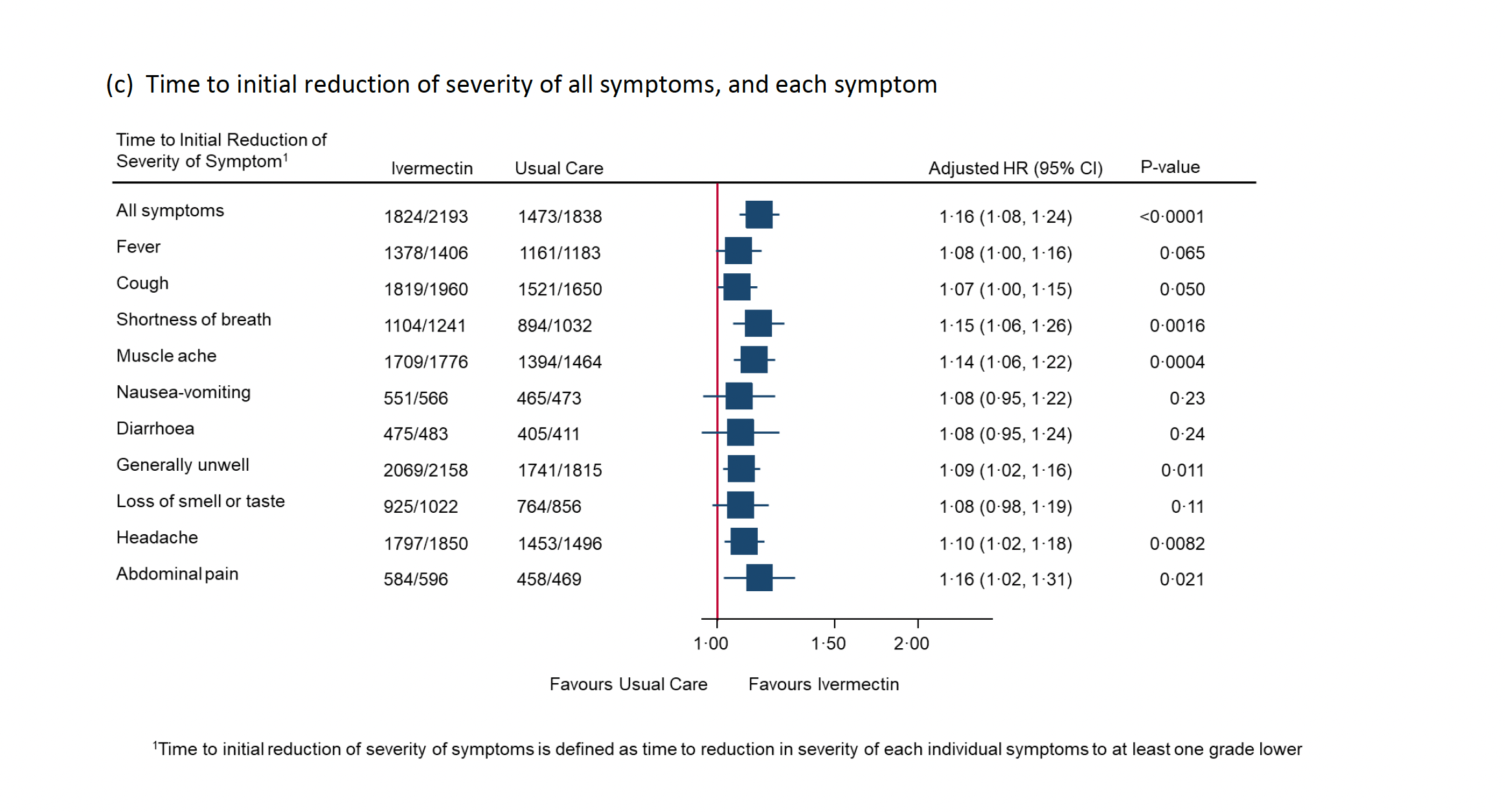
Meanwhile, the report’s appendix includes dozens of recorded clinical benefits in patients treated with ivermectin, such as the time it took to alleviate all symptoms, general unwellness, muscle aches, and headaches. The improvement of symptoms was also sustained, and the severity was reduced. Surprisingly, the source PDF was removed from the website during the writing of this article.
{kind=link}
{kind=link}
{kind=link}
There are additional examples. Although the previously mentioned 2021 JAMA study underdosed patients, treatment with ivermectin reduced recovery time by two days. In the ACTIV-6 study, only one venous blood clot event was reported in 817 ivermectin-treated patients, compared to five events in 774 placebo-treated patients.
Statistical Failures
It is important to note that the definition of treatment effects in an RCT can differ from those discussed in real-life observational studies.
Sometimes, even if the results of a clinical trial demonstrate a clear effect, the conclusion may still be interpreted as ineffective due to the statistical definition of effectiveness.
Interpreting statistics can be challenging as they usually involve complicated mathematical models and numerical data that can be manipulated to support a specific agenda. Nevertheless, for the purpose of this discussion, let’s presume that all research is carried out conscientiously and without manipulative intent.
In a randomized, double-blind, placebo-controlled clinical trial with mild to moderate COVID-19 patients, none of the 55 patients in the ivermectin group died, whereas four of 57 in the placebo group died. This resulted in a comparison of zero percent versus 7 percent. Moreover, only 1.8 percent of ivermectin-treated patients needed invasive ventilation compared to 8.8 percent in the placebo group.
In other words, ivermectin reduced the risk of death by 100 percent and the need for ventilators by 80 percent.
However, the article did not provide the p-value (probability value) for the death rate comparison or the invasive ventilation of 0.102 (Table 2), which is higher than the 0.05 threshold considered to be a significant statistical difference.
P-values are commonly used to test and measure a “null hypothesis,” which states that no differences exist in the effects being studied between two groups. A finding is considered statistically significant and warrants publication when the p-value is 0.05 or less.
The p-values in this study were deemed insignificant because they were more than 0.05. Accordingly, the authors wrote that this difference was statistically insignificant and concluded that ivermectin “had shown only marginal benefit.”
How could a 100 percent reduction in death or an 80 percent reduction in ventilation be interpreted as “marginal” effects?
In the I-TECH study published in JAMA Internal Medicine in 2022, the patients treated with ivermectin had a lower mortality rate of 1.2 percent compared to 4 percent in the comparator group.
The same conclusion was made as the previous study because the p-value was 0.09 and higher than 0.05.
If the 7 million patients reported to have died from COVID-19 had been treated with ivermectin, an estimated 4.9 million lives could potentially have been saved based on the 70 percent reduced mortality rate from the I-TECH study; or 4.5 million lives could have been saved based on the 64 percent reduction of mortality in the PRINCIPLE study.
The life-saving potential of ivermectin has been hindered by the unnecessary statistical threshold. The problem of statistical significance is widespread and frequently causes confusion among scientists.
A 2016 Nature article raised concerns about the misuse of p-values. A 2019 comment in the same journal stated that “The misuse of statistical significance has done much harm to the scientific community and those who rely on scientific advice.”
The authors called for abandoning the use of statistical significance to draw conclusions regarding the effectiveness of drugs, such as stating that “drug Y does not work,” and cautioned that such conclusions may result in the dismissal of potentially life-saving drugs.
The authors also wrote: “Let’s be clear about what must stop; we should never conclude there is ‘no difference’ or ‘no association’ just because a P value is larger than a threshold such as 0.o5.”
Selection Bias
Many people, including physicians, may not be aware that interventional studies, particularly RCTs, are are prone to numerous biases, with selection bias being one of the most significant. Excluding potentially eligible individuals due to their anticipated group allocation can lead to selection bias.
It’s common knowledge that early treatment of COVID-19 is crucial for effective results. The earlier the treatment starts, the more effective it is. These approved antivirals for COVID-19 are used shortly after COVID-19 infection and usually within a few days after symptom onset.
For example, Paxlovid and molnupiravir registration trials treated patients within only three to five days of symptom onset.
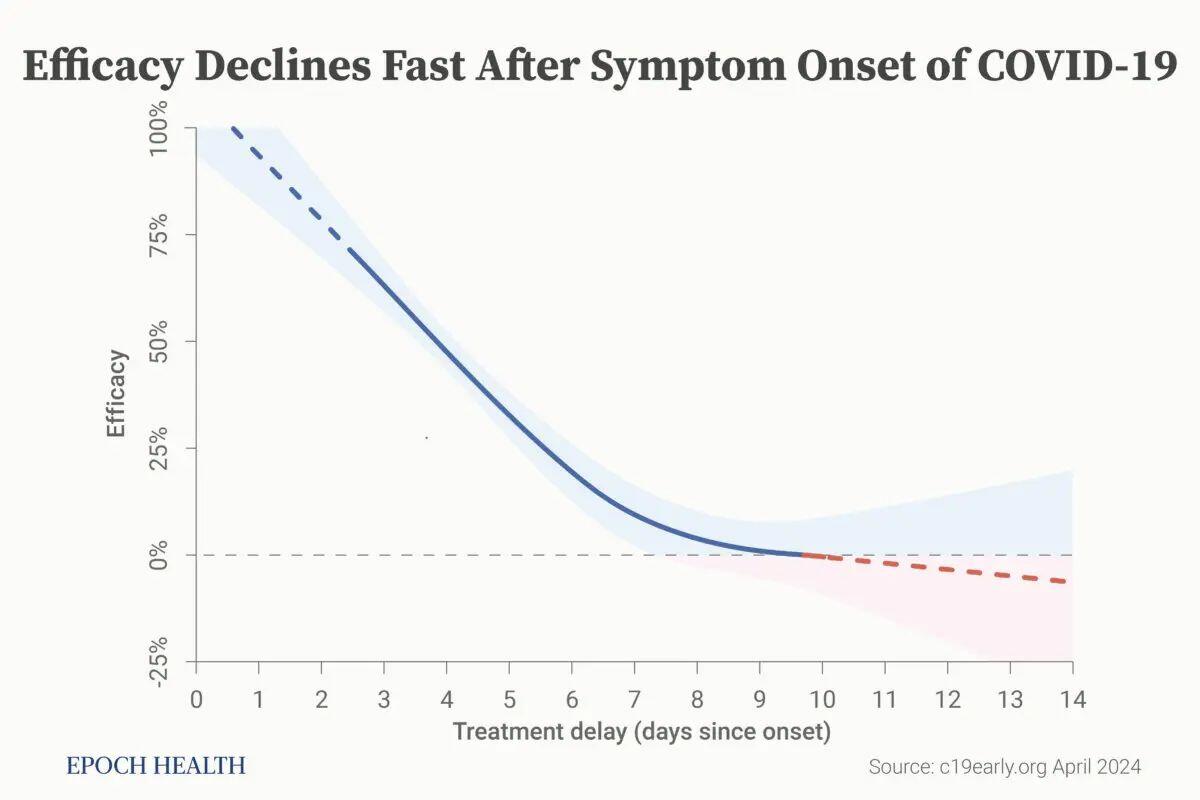
However, in the PRINCIPLE trial, ivermectin was used for patients within 14 days of symptom onset, while ACTIV-6 treated patients an average of six days after infection.
Patients with severe kidney disease are normally excluded from phase 3 studies, as they are less likely to respond to antiviral treatment. This approach has been taken by remdesivir (protocol), molnupiravir (protocol), and Paxlovid (protocol). However, such standard exclusion criteria were not taken by the ACTIV-6 or PRINCIPLE study protocols.
Why was ivermectin treated so unfairly in these clinical trials?
It is well known that when an RCT is sponsored by Big Pharma, there is often a financial conflict of interest, as the research institutions are usually hired or funded by the pharmaceutical company. In a world where wealth often competes with ethics, how many can resist financial temptation and stay true to moral principles?
“Hidden agenda bias” occurs when a trial is conducted to demonstrate a desired outcome, rather than to answer a question. In other words, “Don’t do a trial if it won’t show you what you want to find.”
Proven Without a Profit Motive
Conducting an RCT to get a drug approved by the FDA requires money. Every drug must be managed by a professional team composed of doctors, database managers, and assistants. Professionals must secure funding, recruit a lead investigator, and find hospitals to conduct the study. An operational team must perform the study, analyze the data, and gain FDA approval.
Since ivermectin is a generic drug that lacks profitable marketing and a pharmaceutical sponsor, it’s challenging to organize and systematically manage its new application with health authorities, data, and customers.
Nevertheless, doctors worldwide have been using ivermectin to help patients and have collected valuable data.
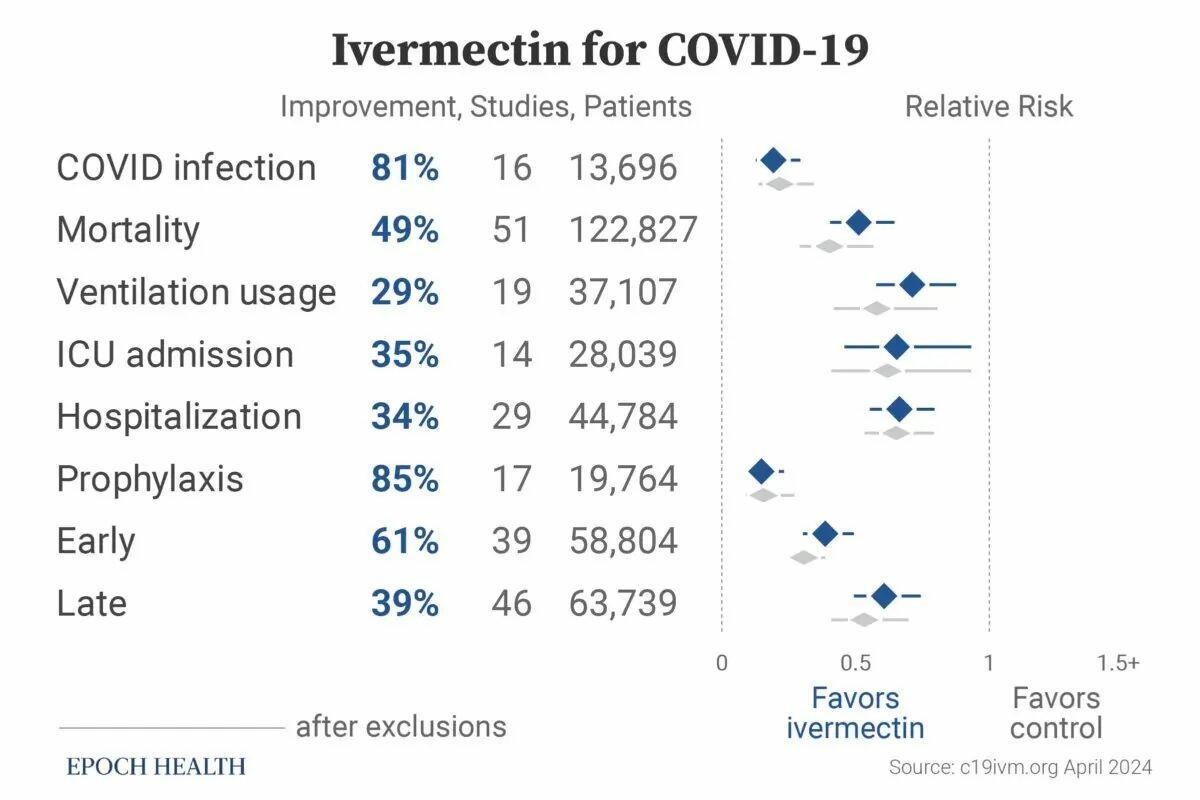
The website c19ivm.org has compiled data on 102 clinical trials proving ivermectin’s consistent effectiveness in treating COVID-19. Studies with negative conclusions about ivermectin are also included, such as the the four RCTs with recognized design flaws.
Since the beginning of the analysis, ivermectin has consistently shown efficacy. This meta-analysis provides a thorough and transparent real-time analysis of all eligible ivermectin studies.
The trials were conducted by 1,139 doctors or scientists from 29 countries with 142,307 patients. Out of the total studies, 86 have been peer-reviewed with 128,787 patients, and 49 were randomized controlled trials with 16,847 patients.
In the studies with comparative groups, ivermectin was shown to reduce the risk of COVID-19 infection by 81 percent, mortality by 49 percent, ICU admission by 35 percent, ventilation usage by 29 percent, and hospitalization by 34 percent.
In comparison to the control groups, the use of ivermectin as a preventive measure before infection reduced the most severe clinical outcomes of COVID-19 by 85 percent. When used in the early stage of COVID-19, ivermectin decreased the severity of the disease by 62 percent, and when used in late stages, it reduced the clinical severity by 39 percent. Clinical severity is measured by death, ventilation, disease progression, or hospitalization.
Considering the Entire Picture
It’s difficult to believe that the designers of these studies were unaware of the dosing of ivermectin. Despite all of the above analyses, the reasoning behind the ivermectin underdosing or unfavorable study design may be linked to factors beyond science.
A new drug or vaccine cannot achieve an Emergency Use Authorization (EUA) status if there is an existing viable therapeutic available. This fact alone may have impacted many decisions.
The NIH website lists only those RCTs that I found to have design flaws (or potential fraud) to justify its recommendation against the use of ivermectin in the treatment of COVID-19.
Peer-reviewed studies showing the efficacy of ivermectin in treating COVID-19 have been retracted without explanation, and doctors have been demonized, censored, and doxxed for speaking the truth.
Legacy media, including The New York Times and CNN, reported incomplete and improperly interpreted trials that failed to present an accurate representation of ivermectin’s effects.
It’s important to keep an open mind and consider the entire picture when examining the ivermectin issue, rather than dismissing it as conspiracy or misinformation. This can lead to more informed decisions that could ultimately save lives.
Views expressed in this article are the opinions of the author and do not necessarily reflect the views of The Epoch Times or ZeroHedge.


What millennials and gen Z professionals need to know about developing a meaningful career


Silver and Gold: The Winning Bet


Tracking ticks in Georgia to help monitor emerging diseases


How the national living wage helps the UK’s poorest households: new research


How Ivermectin Trials Were Designed To Fail


Immigration And Its Impact On Employment


New government guidance for PE lets teachers and pupils down


A small robot car can reduce children’s stress before surgery


CDC Hid Finding Of Possible Link Between COVID Vaccines and Tinnitus


Here is why an airline is trolling Sydney Sweeney
-

 International3 weeks ago
International3 weeks agoParexel CEO to retire; CAR-T maker AffyImmune promotes business leader to chief executive
-

 Spread & Containment1 month ago
Spread & Containment1 month agoIFM’s Hat Trick and Reflections On Option-To-Buy M&A
-

 Government5 days ago
Government5 days agoClimate-Con & The Media-Censorship Complex – Part 1
-

 International1 month ago
International1 month agoWalmart launches clever answer to Target’s new membership program
-

 Spread & Containment3 days ago
Spread & Containment3 days agoFDA Finally Takes Down Ivermectin Posts After Settlement
-

 Uncategorized1 week ago
Uncategorized1 week agoVaccinated People Show Long COVID-Like Symptoms With Detectable Spike Proteins: Preprint Study
-

 Uncategorized7 days ago
Uncategorized7 days agoCan language models read the genome? This one decoded mRNA to make better vaccines.
-

 Uncategorized4 days ago
Uncategorized4 days agoWhat’s So Great About The Great Reset, Great Taking, Great Replacement, Great Deflation, & Next Great Depression?