This article was originally published by ValueWalk.
First on CNBC: CNBC Transcript: Pfizer Chairman and CEO Albert Bourla speaks with CNBC’s “Squawk Box” today, discussing the manufacturing, distributing and efficacy Covid-19 vaccine.
Get The Full Seth Klarman Series in PDF
Get the entire 10-part series on Seth Klarman in PDF. Save it to your desktop, read it on your tablet, or email to your colleagues.
Q3 2020 hedge fund letters, conferences and more
Following is the unofficial transcript of a CNBC interview with Pfizer Chairman and CEO
Albert Bourla on CNBC’s “Squawk Box” (M-F, 6AM-9AM ET) today, Monday, November 9
th. Following are links to video on CNBC.com:
Pfizer CEO Albert Bourla on Covid vaccine efficacy: 'It is a great day for humanity'
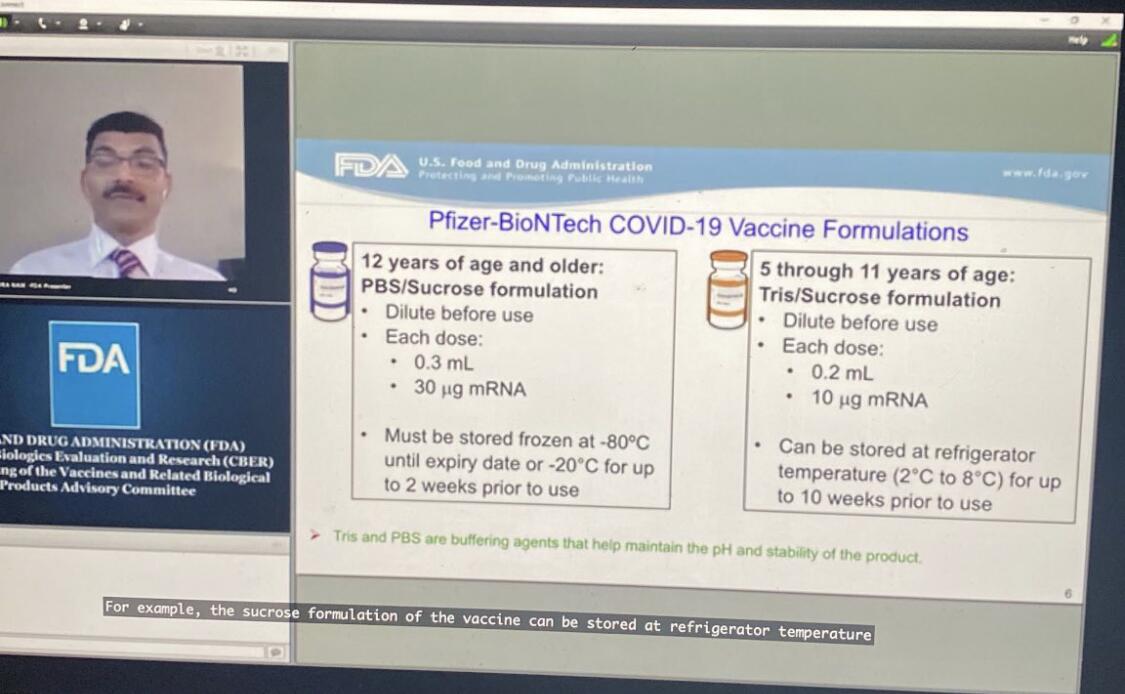
On formulating Covid-19 vaccine for younger and older populations
Pfizer CEO on manufacturing and distributing Covid-19 vaccine
Bourla wants to be among the first to take coronavirus vaccine to allay concerns
BECKY QUICK: Meg Tirrell has a very special guest this morning, Meg This is the news of the morning the news of the week, and much more than that, go ahead and take this away we are all ears.
MEG TIRRELL: Becky, thank you. That guest is Albert Bourla CEO of Pfizer Albert. Thanks for being here. What a morning, I can only imagine what you all at Pfizer are feeling today. What was it like when you saw the results 90% advocacy for your
vaccine for COVID.
ALBERT BOURLA: It was exactly what you can imagine. It is a great day for science. It is a great day for humanity. When you realize that your vaccine has a 90% effectiveness. That’s overwhelming. You understand that the hopes of billions of people and millions and businesses and hundreds of governments that were felt on our shoulders. Now, we can credibly tell them. I think we can see the light at the end of the tunnel.
TIRRELL: You said no serious safety concerns that you've observed in the trial so far. Tell us what you've seen there what's it going to be like for people. If and when this vaccine gets on the market to take these shots I mean, after the second one you do feel some side effects sometimes right.
ALBERT BOURLA: Yes, we have published as you remember, in our r&d day at Pfizer unblinded safety data from the first I think 6000 patients now we have 36,000, almost 40,000 patients with second dose already been given. And it's exactly the same situation hasn’t changed at all so the vulnerability profile. It is among the best.
TIRRELL: So, this is of course just the top line data you took a look in at on an interim basis, you had 94 infections in the trial so we don't have the spelled out data, but what can you tell us about you know did you prevent severe infection in the trial, you know, just tell us what you can essentially at this point about what you know.
ALBERT BOURLA: I am telling you what I can because I don't have this information as you know all this information is blinded then there is a committee of independent experts, that are reviewing the data, according to the protocol, the only information that they had to give us was, if the product is effective and the effectiveness of this product in the first primary endpoint but was people without prior infections. And also they had a look on their safety database, and they told us that they have no safety concerns. We are not even aware of the secondary endpoints, and one of them it is the severe covid, and we are just waiting for the study to be completed but given how quickly the events are occurring because unfortunately this great news are coming at the time that the world needs it. The most where we have hundred thousand cases every day. We will have completed the study I think before the end of the month.
ANDREW ROSS SORKIN: Albert.
Congratulations. I think a lot of people are are. This sigh of relief. Hopefully, and praying that this can get out quickly. One of the issues we've been talking about is the supply constraints and how quickly that's going to change and move I know there's 50 million, doses available before the end of the year 1.2 million doses in calendar year 2021, can you speak to how you see that rolling out is that in fits and starts. How quickly does that come is that by the first half of the year second half of the year, what does that look like.
ALBERT BOURLA: Yeah, thank you very much and first of all let me tell you that there is no one more relieved than me. Seeing this result. And we are already started manufacturing some time back. And as I said, we believe we should be able to have up to 50 million this year, 1.3 billion next year. These two were becoming gradually in the beginning, a little bit less than the first quarter more of a second quarter more. And then we have a significant ramp up in the second half of the year, deliver the 1.3 billion, but given how effective this Covid vaccine is. And we are aware about the demand will be much higher than anything we can produce. We are also looking right now to see if there are other ways thinking out of the box that increased even further. The manufacturing capacity now we're speaking about 1000 people dying in the US, every day right so there's no time to be lost here.
SORKIN: And just to follow up on that the 1.3 doses, a billion doses, I should say, because there are two doses required for each person we're talking really about 650 million people that can be treated is that is that the way to think about it
ALBERT BOURLA: This is exactly the way you think about.
SORKIN: And then the last question I had related to all of this is obviously there are rivals and competitors working on Covid vaccines, and I know you can't speak necessarily to their vaccine efforts, but given what you think you've learned here. Do you think you could extrapolate out those kinds of results in any of this similarly situated. Situated vaccines that are using similar technologies.
ALBERT BOURLA: Well let me tell you when it comes to pandemic. The only competitor is the virus and time. And right now, the first of all of us was able to beat, and I hope that others will also be able to beat this virus, as effectively as we do because we need to, And let me take also the time right now to thank, not only the hundreds, thousands of scientists that work, investigators in this site but more importantly, the 44,000 volunteers that raise their hand to participate in a trial, but they didn't know if the Covid vaccine works, or even if the vaccine is safe. I think the world owes them, big time.
QUICK: Yeah. Hey, Albert I said at the beginning that this is the news of the morning the news of the week but you know forget the election, this is the news of the year this is the most important thing that we've heard the most exciting thing that we've heard. And I just want to thank you, your team. Everybody that you just thanked for this. I mean, this gives us hope that we didn't think was possible just an hour ago. Let me ask you, sign me up for this thing how quickly can you reformulate it and find out what you need to do for older cohorts where, you know, they're most at risk for this or for kids I know, Meg had mentioned earlier that you're doing this for kids as young as 12 right now how quickly can we sign up all of our kids for this how quickly can you get that testing taken care of.
ALBERT BOURLA: The study we're doing all the way from 12 years old to 85, years old so we are collecting data and information for all the age cohorts. We are also doing for people that have chronic diseases, HIV, hepatitis C Hepatitis B. So we will have a lot of data to provide a person of course they will decide which ages, they're going to recommend it, but the study is very robust right now.
QUICK: Yeah, I hate to keep pushing this but I've got a four year old a nine year old and a 94 year old grandmother How quickly can you move beyond that you think are we talking six months we talking nine months.
ALBERT BOURLA: I think about the older people more than 85 I think the likely regulators in cases that they're doing studies to 85 they are giving in physicians, they are trading, very easily for the older people but that's up to physicians simply FDA, of course. And right now we are focusing on the 12 years on but we will do also pediatric, I think the most vulnerable are the older people.
JOE KERNEN: Hey Albert, I got three or four questions. I want to start just, you know you're, it's hard for you to, to be just, you know, very serious and state about this. I can see how happy and excited you are but can I ask you when you heard 90%, was there ever a period in the development where you were questioning whether there would be efficacy? And when you heard that it was 90%, or were you surprised that it was that that high? Were there, do you think that looking at the science, it seems like a really high number that even, it may have surprised you.
ALBERT BOURLA: For some of it you’re right, I'm very happy but at the same time sometimes I have tears in my eyes when I realized that this is the end of the nine months, day and night work of so many people and how many as I said people, billions invested hopes on this. You know, I was going up and down and while I was trying to maintain my mind not to speculate if the Covid vaccine works and then the other day I was thinking maybe it would not because I have seen many times, although the data, your phase one and phase two are very positive, sometimes you fail on phase three. But I was cautiously optimistic. I never thought it would be 90%. That surprised me.
KERNEN: My next question has to do with, it's 90% that's like measles, what we said it's like, that's like a Covid vaccine that we think of that you get when you're a kid and you're done for life. And I'm wondering when will we know whether that's the case? What type of additional studies need to be performed for us to know that there won't be a yearly comeback of a different variation of COVID that would require a flu type shot every year? When will we know how long the immunity lasts in terms of, of
antibodies being present or the right type of cells and what kind of tests are you planning are your scientists planning now that you need to do to determine the answer to those things?
ALBERT BOURLA: Yes, we have already in our protocol provisions that this study will continue and we will follow the patients for two years. And the reason is we want to maintain but for two years that will be, we will exhaust every single possibility but we will pick up any safe event, but also we will see how long the immunogenicity lasts, and how long the cell immunity lasts. And so with this study as time progresses, we will find out about the, the durability of the protection.
QUICK: I said before, sign me up and I'm sure there are lots and lots of people who are thinking the same thing but the ethics of how you distribute this are going to be pretty closely watched. How do you do it, how do you determine who gets it, and who has wait?
ALBERT BOURLA: You're absolutely right and I truly believe that it is not for Pfizer to decide who would get the Covid vaccine. I think it is for the health authorities of every country and in many cases within the same country of every region or of every
state in the US, for example, because the situation differs from state to state or from country to country, and you need to tailor it to the needs of the specific geographical region. We will of course work with all these health authorities to provide them the insight that they need to understand how our product works in groups of other people, in groups of younger people. We will provide all this information and then eventually they have to make the decision, who gets it. Obviously, I believe that all these authorities will make the decisions in the more scientific and equitable ways.
TIRRELL: Hey Albert, it's Meg Tirrell, just to follow up on that question. Of course, you know, governments will be making the decisions about allocation for their citizens but how did the decisions get made about how to allocate the vaccines to different governments? You've made supply agreements around the world. How will Pfizer decide who gets how much the Covid vaccine first versus the US, Europe, Asia, you know, all of these different questions?
ALBERT BOURLA: Yeah, first of all, we have two separate manufacturing lines, one it is in the US, and that has three manufacturing sites in Massachusetts, in Missouri, and in Kalamazoo, Michigan. And we have a separate line in Europe with manufacturing sites in Germany and Belgium. So, we'll be producing in parallel. We have offered this Covid vaccine, and we have signed already contracts to multiple governments in the world and in most cases we define how these quantities will come month after month, all the way to 2021. And we do that proportionally to all of them.
QUICK: Can you break that down at all, Albert, just to give us an example of it is most of the Covid vaccine that's being produced in each of those nations staying in those nations or does it go out dependent on who signed up like what's the breakdown for each of the governments you've already agreed to in terms of who gets what?
ALBERT BOURLA: I think is very, very important but will not stay where they're manufactured, but we will send them to the entire world because you are as protected in a pandemic as your neighbor is protected. We need to understand that. Nevertheless, we have to manufacture in life and facilitate in fairness so I hope that we will be able to see the entire world from these manufacturing sites, and without problems.
KERNEN: So Albert, when was it clear to you? When did, when did you get the actual news, was it just yesterday or was it over the weekend, what was the actual time?
ALBERT BOURLA: It was yesterday afternoon. It was around two o'clock.
KERNEN: Amazing the timing of everything. I just, guys, I just, Albert, I was going to say it has nothing to do with you and I just said I wonder how
Zoom Communications is doing. It closed at 500, it's bidding 440 right now so it's going to be, Albert, it changes a lot of different things I think, just the way that we think about, you know, travel, and we've talked about all these things and I don't want to, I don't want everything to get ahead of itself and I'm wondering, what are we missing in terms of, of something that could pop our bubble down the road? is there anything you can think of that, that could come out, anything that the other than supply issues which we've heard about again and again and again?
ALBERT BOURLA: I think that, that this was very important but only the first step. And now we feel very, very, very confident about the efficacy because it's overwhelming. We feel very good about safety but we need to wait until next week when the safety data will mature completely based on the guidelines of FDA. And of course, we need to make sure that we can constantly manufacture in both, in both continents in Europe and in the US, in the quantities that we are saying, we feel good about all of that.
But of course, as you said before, this is something that has done first time in the world I believe this is likely the most significant medical advance in the last hundred years, right, if you count the impact that this will have in health of the public health, global economy, etc. etc. So I'm happy that we have the whole Pfizer machine and of course biotechs are partners machines behind this and we will be able to support it, I hope.
TIRRELL: Albert, it's Meg Tirrell again. You know we've talked so many times about the timing of this data, and it was so tied to election day. You had expected you would see by the end of October, whether the Covid vaccine worked, you're getting this news now a week after the election. What do you say if
President Trump accuses you of waiting until after the election to release this information?
ALBERT BOURLA: For us, the Election Day was always an artificial date. We were not working with the election as a timeline. We were working, i.e. released a letter, if you remember, Meg, to our employees some time ago, saying that the only pressure we feel it is the pressure of the billions of people that are hoping on our Covid vaccine. And we are going to follow the speed of science so science spoke, and I was predicting that this will happen at the end of October, it happened a week later. I think the most important thing right now for everyone it is to feel the joy that it happened and it happened so well. 90%.
QUICK: Hey Albert, 90% effective is amazing. Oh.
ALBERT BOURLA: I know.
QUICK: 90% is just amazing. I know that again for people who haven't been listening through this entire thing for the flu vaccine it's generally 40 to 60% effective, but I just wonder for the 10% that it's ineffective with, is there a pattern? Can you determine if there's some commonality for the people that doesn't work in?
ALBERT BOURLA: It is too early because as I said I don't have visibility to all the data, it is a group of independent experts, but they can see those data, unblinded. And once we have started completely unblinded but I think will happen at the end, before the end of November. And also keep in mind, I said that it is more than 90%, I didn't say it is 90%.
SORKIN: Oh okay, that's even better.
QUICK: More than 90.
KERNEN: Albert, it is dependent. It is…
ALBERT BOURLA: We will not give a specific number because you know the numbers from 90 to 164 may change one, two points, up or down right so, but right now I feel comfortable it is more than 90%.
KERNEN: But it is dependent on a patient's immune system, own immune system, so I'm wondering, it can you be so immune compromised for whatever reason that it, that it's not effective and is it more effective in, in people with vibrant immune system younger people, people that don't have comorbidities with you, or does it seem across the board, in terms of effectiveness?
ALBERT BOURLA: I believe, yes, in biology, you'll never have hundred percent. And in general, speaking about more than 90% is one of the highest results that you can hope and expect for vaccines, right now, and there will be also, some people, but will be a small percentage. So when you see it from public health perspective, this is more than what you could ever hope to have. This is a game changer.
KERNEN: I wonder, and I wonder what else we can, why can't we, I guess the coronavirus that causes the common cold mutates so quickly that it's impossible to have something that lasts year to year. I'm just trying to understand the difference between maybe some other chronic recurring seasonal diseases that we have and why this new technology couldn't be applied to that or whether it can be applied to some of those things do you know at this point, Albert?
ALBERT BOURLA: Look, I mean, speaking about mutations of coronavirus, I think that this is a likelihood scenario. We start seeing some of them – right now looks like our vaccine is, as I said, very effective for all the mutations that exist out there right now. But in case that a new mutation that requires – let's say new vaccine emerges in one or two years – the good thing with this technology is that you can adapt to technology extremely quickly. Because as you were saying before, you're sending a message to yourselves to produce DNA. It’s an RNA message that you're sending. So, we can just change the code in our Covid vaccine without changing manufacturing process, without changing virtually anything and then being able to be effective against the new mutation. So that's why we selected this technology.
When we started back in March, we had access as Pfizer to multiple platforms of technology. And our scientists proposed me and they selected to use this one for these reasons. You can boost as much as you want. For example, if you need to boost next year, you can do it because this technology allows you to do it and you can do it the year after. So you can have every year a revaccination. And also, if there is a mutation, you can produce in weeks, rather than months a new vaccine.
TIRRELL: Hey, Albert it's Meg Tirrell again. I just want to follow up on the international allocation of this vaccine, because it does seem like it could be a tricky situation. So to make sure we understand, Pfizer is going to be making the decisions about where the Covid vaccine goes country by country. And what about low income nations? Does Pfizer have an agreement with COVAX the facility through the World Health Organization? I mean, do we need some kind of international overseer of
distribution or will companies be making these decisions?
ALBERT BOURLA: Right now, Pfizer has agreements with multiple governments, but also has discussions with even more. And we are, of course, in discussions with COVAX facility and offer to the COVAX facility to provide our Covid vaccine to the low income countries – these are the poorest countries of the world – at the non-for-profit base for these countries. So, we are discussing as we speak, and I hope that we will be able to provide equitable protection to the entire world.
SORKIN: Albert, as you've been speaking, the current president, President Trump tweeting out “Stock market up big, vaccine coming soon. Report 90% effective. Such great news!” My question to you is, given the polling around Americans willingness to take the vaccine, you're seeing some polls suggest somewhere between one-third and two-thirds of Americans say that they won't take the Covid vaccine. What do you think has to happen, what do you think the industry and government needs to do to create the kind of confidence that you'd want to see so that much of the country – if not all of the country – ultimately takes it?
ALBERT BOURLA: Yeah, I think the number one and most important thing is that we keep discussing about the vaccines from scientific and nonpolitical terms. I think this is what confuses people and makes them doubt. They don't know whom and what to believe. The second is what we are already doing and we should continue doing it until the end, which is transparency.
I believe that we were very transparent with our protocols, we were very transparent with our safety data, we are extremely fast to announce their efficacy data once we have them. We believe that it's good that those data will be publicly exposed. I think FDA already plans to have a committee of external advisors to FDA, but they will review the data publicly. And of course I think it is up to the greatest scientists that we have right now in the world – and in the U.S. – to express their opinion about this Covid vaccine. I understand those that they were confused and skeptical about the vaccine, but I need to repeat the decision to vaccinate is not affecting only yourself it is affecting the health of others.
And likely the most vulnerable others. So because if you decide not to vaccinate, you will become the weak link that will allow this virus to replicate and produce the detrimental effects. Which means so many people unemployed, 1,000 deaths every day in the U.S. only and even more in the world – much more in the world. So it's an important decision, but I want everyone to be open minded. From our perspective, we'll do everything we can to convince them that 170 years of legacy is something that we count as Pfizer and plan to respect.
TIRRELL: Albert, some questions for you just about some of the nitty gritty details you put there in the release and we, of course don't have the full data, but one of the details you included is that this 90% efficacy threshold was met in people who did not have evidence of prior infection with SARS-CoV-2. Now you are continuing to evaluate both people who do have prior infection and who don't, to see you know, does it work for everybody. But what scientifically does that potentially mean? You know, would people need get an antibody test before they get this Covid vaccine? Just tell us about that detail and its significance.
ALBERT BOURLA: No, I don't think – of course it's up to FDA and their thoughts, but I don't think really. The first primary endpoint is the only point that external experts were allowed by protocol to talk to us. But of course, they have data about also people that have been previously infected than more by people without taking into consideration if they were previously infected.
That we will only know when the study is complete. But typically it's a lesser hurdle. So if you are able to protect people that were not previously infected, likely you will have better chances to protect people that were. Also we are going to see information that we are going to have for 14 days after vaccination because, keep in mind, right now we use the most extreme test for this Covid vaccine. We tested people seven days after the second injection.
This means that we tested if people can be protected, four weeks after they start their vaccination schedule. First dose day one, 28 days we start looking for effects. It's very, very quick and this is a very, very big test. We are testing also, what happens in 14 days after the second dose, which we expect would be an easier hurdle, but of course we need to see.
SORKIN: Hey, Albert. Back to the confidence point about getting Americans and those around the world to take this. Under what circumstances would you take the vaccine? How quickly would you imagine that you would do it? And if it wasn't the Pfizer Covid vaccine, if it was another company's vaccine, what would you need to see personally for your family to decide to take that vaccine?
ALBERT BOURLA: FDA approves it in the U.S. as we live. And if I was living in Europe, that the European authorities approve it. I truly believe in the integrity and scientific capabilities, first of all, of FDA – that is a renowned agency for this capabilities, but also the European agencies. Once they approve it, I know that it is safe for my family. Myself, I would like very much to get it among the first, so that we can demonstrate to the world that I am the first one.
But I will try it with my family. We need to see some ethical considerations. If, for example, we have a limited number of doses, I don't know if the government would recommend people of my age and my – I mean CDC – people of my age or work capacity to be among the first to get to the vaccine, so I want to respect that. But I will try to convince them to allow me to participate.
TIRRELL: Well, Albert Bourla. This has been a historic morning. We appreciate you being here with us. I can only imagine the pride that your scientists and your entire team feel there at Pfizer. And we are, you know, we see light at the end of the tunnel. So thank you very much for being here with us this morning.
ALBERT BOURLA: Thank you very much for having me.
The post
Pfizer CEO Albert Bourla On Covid-19 Vaccine Efficacy appeared first on
ValueWalk.













































{kind=link}