When the coronavirus pandemic first hit the UK, thousands of surgical procedures were put on hold. For a surgeon like me who performs operations on deaf children to restore their hearing, this created a significant moral dilemma – I wanted to get back into surgery to provide this vital care, but I didn’t want to inadvertently catch or pass on COVID-19 in the process.
I regularly carry out cochlear implant surgery, a process in which a surgeon embeds an electronic device which stimulates the hearing nerve in the ear. The scientific evidence is clear that this surgery needs to be performed at the earliest opportunity so that these children can benefit from being able to hear at a vital stage in their development.
But performing the surgery as normal would have put both children and surgical teams in danger. We needed to come up with another way of doing things. Our team in Nottingham had to combine creativity and science to develop a novel and safe way to restart cochlear implant surgery in a matter of just a few weeks.
This article is part of Conversation Insights The Insights team generates long-form journalism derived from interdisciplinary research. The team is working with academics from different backgrounds who have been engaged in projects aimed at tackling societal and scientific challenges.
A grave risk
Soon after the pandemic began, some of the earliest reports, notably those from China and Italy, suggested that healthcare workers were at significantly higher risk of contracting COVID-19 compared to the general public, and that treating ear, nose and throat (ENT) conditions was particularly risky.
I was deeply saddened when I was told that the one of the first healthcare workers in the UK to die of COVID-19 was Amged El-Hawrani, a 55-year-old ENT colleague from the university hospitals of Derby and Burton. El-Hawrani succumbed to this dreadful disease on March 28 in Leicester’s Glenfield hospital. Although I never had the pleasure of meeting him, his passing was a huge shock to us all. And his exposure to the virus during his care for his patients was a stark reminder of the brutality of this disease.
Like other ENT departments across the world, our service at Nottingham University Hospitals NHS Trust initially halted all elective procedures in March when the pandemic hit the UK, so we could concentrate our team’s efforts on the management of our sickest patients, including those conditions requiring emergency admission, and our cancer services.
Although this initial response proved effective, we were aware that we were not meeting the needs of other patients with time-critical, albeit not life-threatening, conditions. These patients included children who are born deaf and need cochlear implant surgery to restore their hearing as quickly as possible to maximise their chances of developing normal speech and language. Delaying cochlear implant surgery can mean these young people usually never recover full speech and language skills.
We know this because a lot of the critical studies that highlighted the importance of early cochlear implantation on speech and language development were performed locally in Nottingham, which is home to a large number of world-leading hearing researchers. The first paediatric cochlear implant surgery in the UK was performed by the Nottingham Auditory Implant Programme (NAIP) which hosts one of the largest children’s cochlear implant services in the UK.
A unique risk to ear surgeons
As a cochlear implant surgeon for NAIP, and a research lead for the Nottingham Biomedical Research Centre, I was devastated that we were not able to provide our deaf children with the care they needed. That said, I will admit that the idea of performing cochlear implant surgery at the start of the COVID-19 outbreak was unnerving.
Cochlear implants can be life-changing for young children, but they need surgery within a specific window to have the best outcomes.mady70/Shutterstock
ENT healthcare workers are particularly at risk of catching coronavirus during surgery because of the unique nature of the parts of the body we focus on. The nose of an infected person contains a significant load of the SARS-CoV-2 virus that causes COVID-19. The nose is directly connected to the middle ear by a small channel called the eustachian tube, and other types of coronaviruses, including the one that causes the common cold, are commonly found in the middle ear. This means it is highly likely that SARS-CoV-2 also exists in the middle ear, though, no one has confirmed this to date.
The virus uses two proteins to enter human cells (ACE2 and TMPRSS2) that are found throughout the lining of the nose. The same proteins are found in the eye, suggesting that eye transmission is very likely. We also know that animals express both these proteins in their ears, again suggesting that SARS-CoV-2 is highly likely to be found there.
The virus is mainly transmitted via large droplets that require relatively close contact with an infected person. It has also been suggested that it can be transmitted via aerosols, much smaller particles that can spread over much longer distances.
Several medical procedures have been classed as “aerosol generating”, including cochlear implant surgery, which involves drilling into the bone behind the ear to access the middle ear. The high-speed drill we use during surgery can spread droplet and aerosol contamination throughout a confined theatre space. These droplets and aerosols will contain a mixture of water, bone, blood, tissue and, potentially, viable viruses.
Fixing the problem
At the beginning of the outbreak, while we knew we needed to restart cochlear implant surgery urgently, we were also extremely aware of the potential risks associated with performing this operation at the height of the pandemic. This problem concerned me greatly. However, I find that the best way to manage concern is though action, and it was at this time that I was very grateful that I work in a city which hosts one of the UK’s largest cochlear implant programmes.
In the matter of just a few days, following just a couple of brief emails, a few phone calls and the odd Zoom meeting, I managed to gather together a team of internationally recognised experts who were all interested in developing a model of cochlear implant surgery that we could follow during the pandemic.
My first port of call was Padraig Kitterick, head of hearing sciences at my university, who generously gave both his time and all the funds we needed to support this crucial work. Next, I contacted my esteemed surgical colleague, Gerry O’Donoghue, who pioneered cochlear implant surgery in the UK. As always Gerry was enthused to be involved. So much so that he also volunteered the expertise of his son, Kevin, who works with us as an anaesthetist in the Queens Medical Centre in Nottingham.
Left to right: Dr Kevin O'Donoghue, Professor Doug Hartley, Professor Gerry O'Donoghue, Dr Padraig Kitterick and Dr Rachael Lawrence.Douglas Hartley, Author provided
I then asked my colleagues from the anatomy facility if I could borrow enough skulls on which we conducted experiments that would help us analyse the risk of spreading droplets while performing surgery. Without a moment’s hesitation, Susan Anderson and her colleague Dominik Siwek replied, yes, of course they would be delighted to help. Likewise, Richard Hague and his colleagues from the faculty of engineering provided us with essential 3D printing services to support our work.
Early one Saturday morning, along with Rachael Lawrence, an academic ENT surgeon in training, I collected the skulls from an otherwise deserted anatomy dissection room on one of the upper levels of the Queens Medical Centre. We carried them to one of the ENT theatres located at the other side of the hospital that had been generously provided by our theatre manager, Laura Mitchell.
Innovation fuel: cupcakes provided by the author’s daughter.Douglas Hartley, Author provided
Once our team was gathered, we got to work, fuelled by delicious cakes that had been baked by my youngest daughter Alice, decorated with rainbows in support for the NHS.
Our first task was to properly visualise the extent of droplet spread during cochlear implant surgery. To do this, we decided to replace the fluid that we normally use to irrigate our high-speed drilling with a fluorescent dye.
By simulating a cochlear implant operation using this setup, we could see where the dye landed and understand whether we could continue carrying out surgery wearing standard personal protective equipment (PPE).
It soon became apparent from the distribution of luminous dye around the theatre that the contaminated droplets could spread more than two metres from the site of drilling in all directions. This not only includes the area that the surgeon works in, but also the nurses, the anaesthetist, and other theatre staff.
How the fluorescent droplets spread from simulated cochlear implant drilling.Douglas Hartley, Author provided
Even worse, we found that droplets easily migrated underneath our full-face visors, the standard recommended PPE for aerosol-generating procedures in the UK. The droplets landed very close to the eyes of the person wearing it. This suggested that a visor offered inadequate protection.
But we were not discouraged. Now we knew the extent of the problem, we were able to work around the clock for the next few weeks until we managed to develop and refine some rather unusual solutions.
Testing PPE
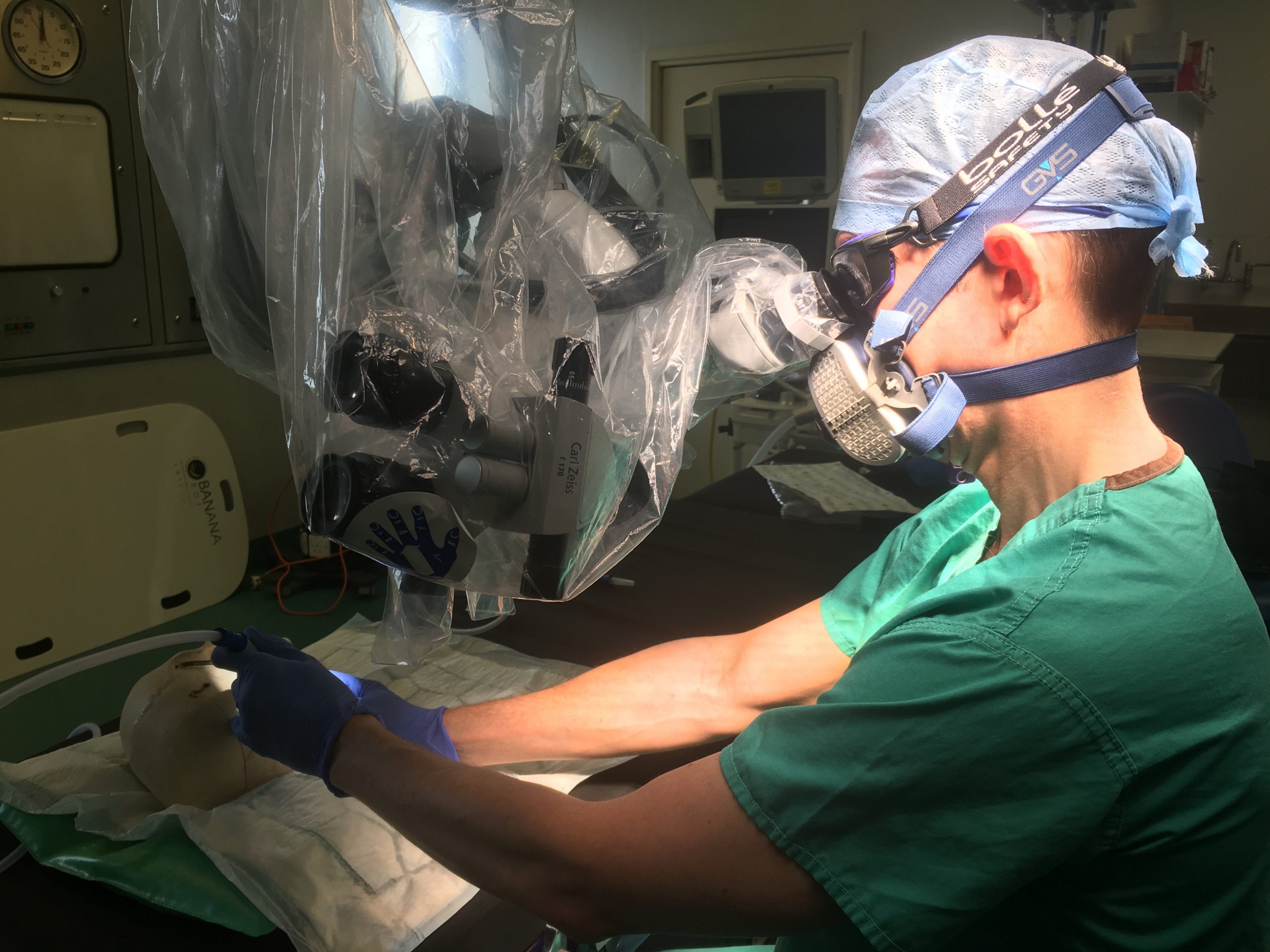
During our studies, we evaluated a variety of PPE options, along with several other infection control solutions. These included a full-face respirator and a combination of a half-face respirator and safety goggles, commonly known as “spoggles”. We had also read reports of teams, including one from Stanford University, who had modified a full-face snorkel mask to be used as PPE, so we tried this too.
The full-face respirator approach.Douglas Hartley, Author provided
We used a systematic evidence-based approach to evaluate the PPE for its usability and effectiveness. During simulated cochlear implant surgery, we evaluated each type of PPE across several parameters, including its effect on a surgeon’s ability to communicate, their field of vision, and their comfort.
Many of the PPE options we tried, not least the full-face respirator, were found to substantially restrict the surgeon’s vision during operating. That rendered them unsafe for performing this sort of surgery. Rather worryingly, we also found that the modified snorkel mask that had been described by various groups on the internet was associated with rebreathing of carbon dioxide, so this was not a viable long-term option for PPE.
The snorkel approach involved re-breathing carbon dioxide, which can be dangerous.Douglas Hartley, Author provided
Instead, we found that the combination of “spoggles” and a half-face respirator mask had consistently superior performance across all aspects of clinical usability compared with all other options.
The spoggles provided the winning solution.Douglas Hartley, Author provided
During our studies, we also worked with a surgical product manufacturer to develop a novel drape, basically a tent, that was designed to be suspended from a microscope covering the patient’s head and torso to provide a physical barrier between the site of drilling and the rest of the team.
We found that the operating tent significantly contained the droplets and prevented them from spreading around the theatre environment. We were the first – and are currently only – group in the world to develop an operating tent design that is marked for medical use. After completing our studies, we now had appropriate PPE and a protective operating tent to permit the safe re-starting of cochlear implant surgery during the pandemic.
Prof Gerry O'Donoghue models the new surgical tent.Douglas Hartley, Author provided
The new surgical normal
Our recommendations were rapidly disseminated internationally via webinars and journal publications and quickly adopted as standard patient care by our hospital trust and, subsequently, embraced in other departments in the UK and across the world.
Locally, it was with huge relief that we recommenced cochlear implant surgery for profoundly deaf children after a few days of completing our studies: just a couple of months after this procedure was put on hold. Operating times were a little longer initially, and for the first few procedures we opted to have a backup surgeon available just in case the primary operating surgeon needed some help using this new setup.
Today, these new measures have become second nature to our theatre team, operating times are comparable to our pre-COVID surgeries, and lists are running as before with just one surgeon operating. Apart from a little discomfort associated with wearing the PPE for long periods of time, and the ongoing detrimental impact of the PPE on communication, we have all pretty much accepted the setup as our new normal. In fact, I would go so far as to say, it would feel a little naked to operate without these measures now.
We have had to find new ways of communicating while wearing PPE.Douglas Hartley, Author provided
The safe recommencement of cochlear implant surgery in Nottingham, and in other centres around the globe, has given many hundreds of deaf children worldwide the chance to hear. These children can grow up with the potential to develop comparable speech and language skills to their peers. Without this timely surgical intervention, life would have been very different for these children and their families.
The value of speed and collaboration
The coronavirus crisis has been a strange and scary time for everyone, and it has presented us all with many significant challenges in how we live and work. But it has also opened a number of doors for new opportunities and possibilities.
Before COVID-19, if you told me that I’d need to construct a tent in which to operate this year, while wearing spoggles and a respirator mask, I would not have believed you. That said, I’m sure that most people would not have predicted how much we have all had to rely on Zoom and other new digital media to facilitate our work and social interactions with others over the past few months.
The process involved to translate a novel idea from the laboratory bench all the way through to implementation at the patient’s bedside is normally a very complicated and lengthy one that can take years, and sometimes decades, to complete. So it has been heartening to witness the value of a team working to solve a problem at breakneck speed, without much need for the phrase: “I don’t think we can do that.” Necessity is truly the mother of invention and, with a bit of luck, some of this innovation spirit will live on beyond the pandemic.
What next?
It seems that COVID-19 is likely to be with us for the foreseeable future. So we have no plans to abandon our PPE and operating tent for cochlear implant surgery any time soon. In fact, there is a strong argument among the surgical community that these measures should always be used to protect the theatre team from potential contaminants, and the patient from exposure to infections in theatre, regardless of the current pandemic.
Other surgical specialities have also been very interested in the operating tent method as an infection prevention control measure, including those that commonly use an operating microscope, such as spinal surgery, ophthalmology and neurosurgery. In the future we may see a wider use of operating tents.
Certainly, our theatre teams face an ongoing problem from the negative impact of PPE on communication during surgery. It goes without saying that communication is critical for the safe functioning of an operating theatre, and this problem needs an urgent solution. That’s why our group and other centres around the world are continuing to work on the design, not only to aid communication, but also to facilitate easy access into the tent for the surgeon and theatre nurses, while keeping the contaminated droplets inside.
Although COVID-19 has presented significant challenges to recommencing cochlear implant surgery, through collaborative teamwork across a wide range of disciplines, we found solutions. As a team we have certainly learnt from this experience; lessons that I hope we will retain far beyond this pandemic.
To hear about new Insights articles, join the hundreds of thousands of people who value The Conversation’s evidence-based news. Subscribe to our newsletter.
Douglas Hartley works for Nottingham University and Nottingham University Hospitals NHS Trust. He receives funding from the National Institute for Health Research, the Medical Research Council, Action on Hearing Loss, Cochlear UK, Advanced Bionics and Rinri Therapeutics.
The U.S. Supreme Court will soon hear oral arguments in a case that concerns what two lower courts found to be a “coordinated campaign” by top Biden administration officials to suppress disfavored views on key public issues such as COVID-19 vaccine side effects and pandemic lockdowns.
The Supreme Court has scheduled a hearing on March 18 in Murthy v. Missouri, which started when the attorneys general of two states, Missouri and Louisiana, filed suit alleging that social media companies such as Facebook were blocking access to their platforms or suppressing posts on controversial subjects.
The initial lawsuit, later modified by an appeals court, accused Biden administration officials of engaging in what amounts to government-led censorship-by-proxy by pressuring social media companies to take down posts or suspend accounts.
Some of the topics that were targeted for downgrade and other censorious actions were voter fraud in the 2020 presidential election, the COVID-19 lab leak theory, vaccine side effects, the social harm of pandemic lockdowns, and the Hunter Biden laptop story.
The plaintiffs argued that high-level federal government officials were the ones pulling the strings of social media censorship by coercing, threatening, and pressuring social media companies to suppress Americans’ free speech.
‘Unrelenting Pressure’
In a landmark ruling, Judge Terry Doughty of the U.S. District Court for the Western District of Louisiana granted a temporary injunction blocking various Biden administration officials and government agencies such as the Department of Justice and FBI from collaborating with big tech firms to censor posts on social media.
Later, the Court of Appeals for the Fifth Circuit agreed with the district court’s ruling, saying it was “correct in its assessment—‘unrelenting pressure’ from certain government officials likely ‘had the intended result of suppressing millions of protected free speech postings by American citizens.’”
The judges wrote, “We see no error or abuse of discretion in that finding.”
The ruling was appealed to the Supreme Court, and on Oct. 20, 2023, the high court agreed to hear the case while also issuing a stay that indefinitely blocked the lower court order restricting the Biden administration’s efforts to censor disfavored social media posts.
Supreme Court Justices Samuel Alito, Neil Gorsuch, and Clarence Thomas would have denied the Biden administration’s application for a stay.
“At this time in the history of our country, what the Court has done, I fear, will be seen by some as giving the Government a green light to use heavy-handed tactics to skew the presentation of views on the medium that increasingly dominates the dissemination of news,” Justice Alito wrote in a dissenting opinion.
The Supreme Court has other social media cases on its docket, including a challenge to Republican-passed laws in Florida and Texas that prohibit large social media companies from removing posts because of the views they express.
Oral arguments were heard on Feb. 26 in the Florida and Texas cases, with debate focusing on the validity of laws that deem social media companies “common carriers,” a status that could allow states to impose utility-style regulations on them and forbid them from discriminating against users based on their political viewpoints.
The tech companies have argued that the laws violate their First Amendment rights.
The Supreme Court is expected to issue a decision in the Florida and Texas cases by June 2024.
‘Far Beyond’ Constitutional
Some of the controversy in Murthy v. Missouri centers on whether the district court’s injunction blocking Biden administration officials and federal agencies from colluding with social media companies to censor posts was overly broad.
In particular, arguments have been raised that the injunction would prevent innocent or borderline government “jawboning,” such as talking to newspapers about the dangers of sharing information that might aid terrorists.
But that argument doesn’t fly, according to Philip Hamburger, CEO of the New Civil Liberties Alliance, which represents most of the individual plaintiffs in Murthy v. Missouri.
In a series of recent statements on the subject, Mr. Hamburger explained why he believes that the Biden administration’s censorship was “far beyond anything that could be constitutional” and that concern about “innocent or borderline” cases is unfounded.
For one, he said that the censorship that is highlighted in Murthy v. Missouri relates to the suppression of speech that was not criminal or unlawful in any way.
Mr. Hamburger also argued that “the government went after lawful speech not in an isolated instance, but repeatedly and systematically as a matter of policy,” which led to the suppression of entire narratives rather than specific instances of expression.
“The government set itself up as the nation’s arbiter of truth—as if it were competent to judge what is misinformation and what is true information,” he wrote.
“In retrospect, it turns out to have suppressed much that was true and promoted much that was false.”
The suppression of reports on the Hunter Biden laptop just before the 2020 presidential election on the premise that it was Russian disinformation, for instance, was later shown to be unfounded.
Some polls show that if voters had been aware of the report, they would have voted differently.
It’s official. Joe Biden and Donald Trump have secured the necessary delegates to be their parties’ nominees for president in the 2024 election. Barring unforeseen events, the two will be formally nominated at the party conventions this summer and face off at the ballot box on Nov. 5.
It’s a safe bet that, as in recent elections, this one will play out largely online and feature a potent blend of news and disinformation delivered over social media. New this year are powerful generative artificial intelligence tools such as ChatGPT and Sora that make it easier to “flood the zone” with propaganda and disinformation and produce convincing deepfakes: words coming from the mouths of politicians that they did not actually say and events replaying before our eyes that did not actually happen.
The result is an increased likelihood of voters being deceived and, perhaps as worrisome, a growing sense that you can’t trust anything you see online. Trump is already taking advantage of the so-called liar’s dividend, the opportunity to discount your actual words and deeds as deepfakes. Trump implied on his Truth Social platform on March 12, 2024, that real videos of him shown by Democratic House members were produced or altered using artificial intelligence.
The Conversation has been covering the latest developments in artificial intelligence that have the potential to undermine democracy. The following is a roundup of some of those articles from our archive.
1. Fake events
The ability to use AI to make convincing fakes is particularly troublesome for producing false evidence of events that never happened. Rochester Institute of Technology computer security researcher Christopher Schwartz has dubbed these situation deepfakes.
“The basic idea and technology of a situation deepfake are the same as with any other deepfake, but with a bolder ambition: to manipulate a real event or invent one from thin air,” he wrote.
Situation deepfakes could be used to boost or undermine a candidate or suppress voter turnout. If you encounter reports on social media of events that are surprising or extraordinary, try to learn more about them from reliable sources, such as fact-checked news reports, peer-reviewed academic articles or interviews with credentialed experts, Schwartz said. Also, recognize that deepfakes can take advantage of what you are inclined to believe.
From the question of what AI-generated disinformation can do follows the question of who has been wielding it. Today’s AI tools put the capacity to produce disinformation in reach for most people, but of particular concern are nations that are adversaries of the United States and other democracies. In particular, Russia, China and Iran have extensive experience with disinformation campaigns and technology.
“There’s a lot more to running a disinformation campaign than generating content,” wrote security expert and Harvard Kennedy School lecturer Bruce Schneier. “The hard part is distribution. A propagandist needs a series of fake accounts on which to post, and others to boost it into the mainstream where it can go viral.”
Russia and China have a history of testing disinformation campaigns on smaller countries, according to Schneier. “Countering new disinformation campaigns requires being able to recognize them, and recognizing them requires looking for and cataloging them now,” he wrote.
But it doesn’t require the resources of shadowy intelligence services in powerful nations to make headlines, as the New Hampshire fake Biden robocall produced and disseminated by two individuals and aimed at dissuading some voters illustrates. That episode prompted the Federal Communications Commission to ban robocalls that use voices generated by artificial intelligence.
AI-powered disinformation campaigns are difficult to counter because they can be delivered over different channels, including robocalls, social media, email, text message and websites, which complicates the digital forensics of tracking down the sources of the disinformation, wrote Joan Donovan, a media and disinformation scholar at Boston University.
“In many ways, AI-enhanced disinformation such as the New Hampshire robocall poses the same problems as every other form of disinformation,” Donovan wrote. “People who use AI to disrupt elections are likely to do what they can to hide their tracks, which is why it’s necessary for the public to remain skeptical about claims that do not come from verified sources, such as local TV news or social media accounts of reputable news organizations.”
AI-powered disinformation campaigns are also difficult to counter because they can include bots – automated social media accounts that pose as real people – and can include online interactions tailored to individuals, potentially over the course of an election and potentially with millions of people.
Harvard political scientist Archon Fung and legal scholar Lawrence Lessig described these capabilities and laid out a hypothetical scenario of national political campaigns wielding these powerful tools.
Attempts to block these machines could run afoul of the free speech protections of the First Amendment, according to Fung and Lessig. “One constitutionally safer, if smaller, step, already adopted in part by European internet regulators and in California, is to prohibit bots from passing themselves off as people,” they wrote. “For example, regulation might require that campaign messages come with disclaimers when the content they contain is generated by machines rather than humans.”
Artificial mucus identifies link to tumor formation
NEW ORLEANS, March 18, 2024 – During cold and flu season, excess mucus is a common, unpleasant symptom of illness, but the slippery substance is essential…
NEW ORLEANS, March 18, 2024 – During cold and flu season, excess mucus is a common, unpleasant symptom of illness, but the slippery substance is essential to human health. To better understand its many roles, researchers synthesized the major component of mucus, the sugar-coated proteins called mucins, and discovered that changing the mucins of healthy cells to resemble those of cancer cells made healthy cells act more cancer-like.
Credit: American Chemical Society
NEW ORLEANS, March 18, 2024 – During cold and flu season, excess mucus is a common, unpleasant symptom of illness, but the slippery substance is essential to human health. To better understand its many roles, researchers synthesized the major component of mucus, the sugar-coated proteins called mucins, and discovered that changing the mucins of healthy cells to resemble those of cancer cells made healthy cells act more cancer-like.
The researcher will present her results today at the spring meeting of the American Chemical Society (ACS). ACS Spring 2024 is a hybrid meeting being held virtually and in person March 17-21; it features nearly 12,000 presentations on a range of science topics.
“For hundreds of years, mucus was considered a waste material or just a simple barrier,” says Jessica Kramer, a professor of biomedical engineering who led the study. And indeed, it does serve as a barrier, regulating the transport of small molecules and particulates to underlying epithelial cells that line the respiratory and digestive tracts. But it also does much more. Studies show that mucus and mucins are biologically active, playing roles in immunity, cell behavior and defense against pathogens and cancer. Kramer’s team at the University of Utah, for example, recently found that specific sugars attached to mucins inhibited coronavirus infection in cell culture.
“Part of the challenge of studying mucus and mucins in general is that they have quite a variety of protein structures,” Kramer explains. Although humans share more than 20 mucin genes, those genes are expressed differently in different tissues and are spliced to generate a range of proteins. In addition, cells modify those proteins in myriad ways with different sugars to meet the body’s needs.
Complicating the picture, genetic factors alone don’t determine mucin composition. Dietary and environmental factors can also influence which sugars become attached to these proteins. Thus, mucus composition can vary significantly from person to person, from day to day, and from tissue to tissue, all of which makes it difficult to identify the biological effects of any given mucin.
To study mucin properties, researchers can collect mucus from animals in slaughterhouses, Kramer says. “But ultimately, it’s quite labor intensive and difficult to purify. And in the process of doing the harvesting, usually the sticky, slimy properties are disrupted.”
As an alternative, mucins can be purchased off-the-shelf, Kramer explains. But because batch-to-batch variability can lead to problems with experimental reproducibility, methods are needed to reliably produce synthetic mucins at scale and at a reasonable price.
In the absence of a simple genetic method to produce individual mucins, Kramer’s lab combined synthetic chemistry and bacterial enzymes to generate the core polypeptides and then selectively add sugars to create unique synthetic mucins. This allows the researchers to test the physical, chemical and biological properties of individual types of mucin molecules and identify the impact of changing individual sugars or protein sequences.
Kramer, along with the lab of collaborator Jody Rosenblatt at King’s College London, is applying her team’s mucins to questions of cancer biology. In particular, the scientists are exploring the influence of mucins on the earliest stages of tumor formation. Previous studies in other labs have shown that mucins embedded in the surface of cancer cells promote metastasis, the spread of cancer to other tissues in the body. These mucins can also help the cancer cells evade immune system defenses by blocking immune cell activation.
“We are building synthetic mucins to understand how the chemical aspects of these proteins affect the behavior of cancer cells,” Kramer explains. “It hasn’t been possible to study these things before because we can’t control the molecular properties of mucins using traditional genetic and biochemical methods.”
Normally, as non-cancerous epithelial cells grow, they crowd together, with some getting eliminated from the epithelial layer to maintain a consistent and stable tissue structure. When Kramer’s team engineered the cells to have a bulky mucin-rich surface similar to that of cancer cells, the cells stopped extruding normally and piled up, forming what looked like the start of tumors.
Kramer is quick to note, however, that her team has not determined whether the genetics of the cells have changed, so they cannot yet state definitively whether the healthy cells were transformed into cancer cells. Those studies are ongoing.
The insights will be pivotal for the development of possible cancer treatments targeting mucins, as they will help highlight which parts of the mucin molecules are most important to tumor formation.
Scientists have been trying to make mucin-targeting therapeutics for decades, but that hasn’t worked well, in part because the sugar groups on the molecules weren’t fully taken into account, Kramer says. “For a vaccine, we can’t only consider the protein sequence because that’s not what the molecule looks like to the immune system. Instead, when an immune cell bumps into the surface of a cancer cell it’s going to see the sugars first, not the protein backbone.” So she believes an effective vaccine will need to target those mucin sugars.
Beyond cancer, the ability to reliably modify the protein sequence and sugars and produce scalable quantities of synthetic mucins offers opportunities to develop these molecules as anti-infectives, probiotics and therapies to support reproductive and women’s health, Kramer says.
The research was funded by the National Institute of General Medical Science, National Science Foundation and Marion Milligan Mason Fund.
Visit the ACS Spring 2024 program to learn more about this presentation, “Synthetic mucins: From new chemical routes to engineered cells,” and more scientific presentations.
###
The American Chemical Society (ACS) is a nonprofit organization chartered by the U.S. Congress. ACS’ mission is to advance the broader chemistry enterprise and its practitioners for the benefit of Earth and all its people. The Society is a global leader in promoting excellence in science education and providing access to chemistry-related information and research through its multiple research solutions, peer-reviewed journals, scientific conferences, eBooks and weekly news periodical Chemical & Engineering News. ACS journals are among the most cited, most trusted and most read within the scientific literature; however, ACS itself does not conduct chemical research. As a leader in scientific information solutions, its CAS division partners with global innovators to accelerate breakthroughs by curating, connecting and analyzing the world’s scientific knowledge. ACS’ main offices are in Washington, D.C., and Columbus, Ohio.
To automatically receive news releases from the American Chemical Society, contact newsroom@acs.org.
Note to journalists: Please report that this research was presented at a meeting of the American Chemical Society. ACS does not conduct research, but publishes and publicizes peer-reviewed scientific studies.
Title
Synthetic mucins: From new chemical routes to engineered cells
Abstract
Mucin glycoproteins are the major component of mucus and the epithelial glycocalyx. Mucins are essential for life, serving roles as a physical barrier, a lubricant, and a biochemical moderator of infection, immunity, and cancer. There are more than 20 known mucin genes with variable expression patterns, splicing, and post-translational glycosylation patterns. Such diversity has challenged study of structure-function relationships. We are developing scalable methods, based on polymerization of amino acid N-carboxyanhydrides, to synthesize glycan-bearing polypeptides that capture the chemical and physical properties of native mucins. We are utilizing these synthetic mucins to form fully synthetic mucus hydrogels and to engineer the glycocalyx of live cells to shed light on the role of glycans in health and disease. This talk will focus on advances in chemical synthesis along with application of synthetic mucins in study of tumorigenesis.
We use cookies on our website to give you the most relevant experience by remembering your preferences and repeat visits. By clicking “Accept”, you consent to the use of ALL the cookies.
This website uses cookies to improve your experience while you navigate through the website. Out of these, the cookies that are categorized as necessary are stored on your browser as they are essential for the working of basic functionalities of the website. We also use third-party cookies that help us analyze and understand how you use this website. These cookies will be stored in your browser only with your consent. You also have the option to opt-out of these cookies. But opting out of some of these cookies may affect your browsing experience.
Necessary cookies are absolutely essential for the website to function properly. These cookies ensure basic functionalities and security features of the website, anonymously.
Cookie
Duration
Description
cookielawinfo-checbox-analytics
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Analytics".
cookielawinfo-checbox-functional
11 months
The cookie is set by GDPR cookie consent to record the user consent for the cookies in the category "Functional".
cookielawinfo-checbox-others
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Other.
cookielawinfo-checkbox-necessary
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookies is used to store the user consent for the cookies in the category "Necessary".
cookielawinfo-checkbox-performance
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Performance".
viewed_cookie_policy
11 months
The cookie is set by the GDPR Cookie Consent plugin and is used to store whether or not user has consented to the use of cookies. It does not store any personal data.
Functional cookies help to perform certain functionalities like sharing the content of the website on social media platforms, collect feedbacks, and other third-party features.
Performance cookies are used to understand and analyze the key performance indexes of the website which helps in delivering a better user experience for the visitors.
Analytical cookies are used to understand how visitors interact with the website. These cookies help provide information on metrics the number of visitors, bounce rate, traffic source, etc.
Advertisement cookies are used to provide visitors with relevant ads and marketing campaigns. These cookies track visitors across websites and collect information to provide customized ads.























































{kind=link}