International
The ABCs of PCR Tests – Kits, Reagents and Viruses
Kits and reagents and viruses
Share this:

This article was originally published by Virology Down Under.
The COVID-19 pandemic has driven use of the words “kit” and “reagent”. I completely feel for you if you still have no real idea of what is meant by these words in any given story. But be confuddled no longer! You will soon be as hip in this lingo of the lab as anyone can be. Let’s explore these terms as they apply to severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) testing, which is all about detecting a tiny bit of the unique genetic sequence that makes this virus different from that virus and different from a cabbage. If it’s present in our respiratory tract swab specimen of course.

The process
Before we get to those two words though, I’m going to walk you through the process we use to test a suspect person’s specimen for SARS-CoV-2 (severe acute respiratory syndrome coronavirus 2), the virus that causes coronavirus disease 2019 (COVID-19).
I’ve thrown together a graphic below. Its intent is just to give you a basic idea of the timing for a single patient’s sample and of the steps involved. Your experience (patient of scientist) may vary.
Of course, a lab doesn’t usually test one sample at a time. There would be some pretty epic delays if we did (and there have been in 2020!). So imagine the difference in the time it takes to make scrambled eggs, toast and coffee for one person versus 3,000 people – all within 10 minutes of them ordering!
You can probably see that these numbers will scale up and some labs will be able to cope with that better than others. Sometimes it’s actually faster to test more than one at a time because of the way testing is done. For example, we could deliver 96 samples to the lab faster in one trip than in 96 single trips. We can also run other steps in batches. But we still have to report out a lot of individual results at the other end, and answer questions. So swings and roundabouts. I’m sure you get the idea.

The sample: extracting the wheat from the chaff
When we test for SARS-CoV-2, we don’t want all the gunk that comes from up your nose or throat or down in your lungs in our testing tube. We just want the virus’s genetic material. Apart from being gluggy and disgusting, that gunk can make our test fail as some of its elements inhibit the enzymatic reaction that is at the heart of our test.
Once a sample has been collected, sent to the lab and logged in, a portion goes on to a different spot in the lab/different lab where we clear out the protein and the carbohydrates and salts and cells and this morning’s breakfast. We call this step nucleic acid “extraction” or “purification”.
NOTE: we get DNA and RNA in this process and all of what I’m talking about here can apply to the process for testing for any of the 200 or so respiratory viruses.
This can be done in different ways but the most common is a multistep process which essentially:
- busts open any cells (human or bacterial) or viruses
- dissolves and washes away the crud while capturing the nucleic acids present from the newly created biological soup
- washes a bit more to get rid of salts and generally rinses
- changes the chemical balance and washes (“elutes”) the now pure nucleic acids into a tiny volume (we may start with 200µl [millionths of a litre] of a sample, finishing up with about 60µl of “extract”
This process can be done by hand – manually – with pipetting steps and centrifugation to remove waste liquids and swapping and discarding of tubes and lots of labelling and so on.
It can also be done in a semi- or fully-automated way using extraction or “liquid-handling” robots.
The best nucleic acid extraction systems let us add the original patients’ sample in one end, walk away (seldom has this been my experience but that may say more about me than the robots) and collect the extract at either end once the process is complete. Robots can be more reliable, use kits that have been made with a quality-assured process, reduce the risk of cross-contaminating one sample with droplets from another, need way less hand-labelling and generally have much higher throughput than the manual process.
This is essential when you have thousands of samples awaiting testing each day and need things to go smoothly, freeing you up to use your big brain on other things.
DIAGNOSTICS vs RESEARCH: Research labs will generally do things manually and swear by that (including making their own extraction reagents ), whereas professional diagnostic labs will use automation whenever they can, and swear by that because quality assurance.
The test: seeking SARS-CoV-2 through amplification
This bit is more technical. We usually take 5µl of the colourless nucleic acids extract then add that to about 15µl of a mix made up of different chemicals, molecules and mixtures (reagents-see below). This we call the ‘reaction mix’.

The reaction mix
In this mix we’ve added primers, a probe labelled with a molecule that can fluoresce when broken off the probe, some buffer, nucleotides (the “building blocks” of the DNA strands we’re about to exponentially make in the tube), an enzyme that makes a DNA copy from an RNA template (which is the SARS-CoV-2’s genetic material) and one that makes lots of DNA (sometimes one enzyme performs both functions) from each newly made DNA copy.
THE ENZYMES: the enzyme we use are called polymerases. These make a copy – a new chain of nucleotide – of a template strand, starting from where a primer is bound, and adding the appropriate complementary nucleotide one after another, in a new growing chain – or DNA strand. We call the lab method that harnesses these enzymes, the polymerase chain reaction, or PCR. When our virus uses RNA to carry around its genetic code, like SARS-CoV-2, we have to add a step to our PCR. We make a DNA copy of the RNA using an RNA-dependent DNA polymerase and add a step called reverse transcription (RT). Not the test is called an RT-PCR.

The enzymes need the primers to bind to their target to set up their copying activities. The probe binds to the newly made DNA chains if the virus is present. If the target virus isn’t present or is there but in too small an amount, the test will return a negative result.
GETTING A LOT FROM MUCH LESS: Compared to what used to be the gold standard for detecting virus from sick patents, growth in permissive cell cultures – the PCR method we used today is hundred to thousands of times more sensitive.
The primer-target and probe-target binding is really specific. If we’ve done our primer and probe design job properly, we won’t get a positive result to a different coronavirus or a virus from a different family of viruses. The version of This is called a real-time (r) reverse transcriptase (RT) polymerase chain reaction (PCR), or RT-rPCR, mix. (I’ve written about PCR and RT-PCR but both blogs need some work)
The primers and probe are designed to match/reflect the sequence of the virus and so it won’t bind well to any different sequence.
Every different thing with a genome is genetically distinct, even different viruses. All the species have unique genetic codes. We design our primers to seek out the unique bits of the SARS-CoV-2 genome (sometimes the sarbecoviruses as a group), but not the same genetic region of, say, HCoV-229E. This is because the sequence in that same region is different between eth two viruses.
This feature makes PCR highly specific to the target of choice. The cyclical nature of PCR makes it highly sensitive.
NOTE We know there’ll be a genetic difference because when we designed out PCR test, we sat down and compared all the viruses in the family, and – as best as we could predict – chose regions that would be unique.

Once we have the primers in the lab, we verify they do what we expect by actually testing other viruses and making sure we get on “false positives”.
How does a “kit” fit in?
Because diagnostic labs need to move samples through at speed and need the process to work and be high quality, they will not spend their time making all the different chemical mixtures needed to extract nucleic acids or the buffers and enzymes and primers and probes used in the PCR mix. The lab will buy them in from companies who specialise in making quality materials over and over and at scale.
We can buy extraction chemicals in a kit. The kit provides everything premade, sometimes prediluted and ready to plug ‘n play. We also need to buy some disposable plasticware like the many (oh so many!) pipette tips that fit onto the automated pipettors and maybe some tubes and other bits and pieces. Then we can add those liquids and plates and troughs and plasticware to the robots and away we go.






We can also buy primers and primers either individually or they can be supplied in kits – where they come pre-made labelled and put in tubes with instructions for how to use them.











Lastly, we can buy PCR or RT-PCR kits – these come with the buffer already containing nucleotides and enzyme, or with them kept separately, sometimes other chemical and usually with some high-grade water.





What is a “reagent”?
A reagent is a term used widely in the lab – basically for anything chemical. A culture flask or a pipette tip sin;t a reagent (we call them consumables it plasticware). A pipette or a bottle isn’t a reagent, they are, well, they’re pipettes and bottles. D’uh.
We use the word for the ingredients in our experiments. They can be pure chemicals or mixtures, powders or crystalline (salts or sugars), or powders. A solid or a liquid. A reagent can be an acid or a base, water, a buffered salt solution or an enzyme in glycerol. In the case of our story, reagents can be individual primers and probes or the mixtures and buffers that make up the extraction kits. The word is pretty broadly used.
What was in short supply early in the COVID-19 pandemic?
About three weeks ago there was lots of talk about COVID-19-related shortages, mostly of “kits”.[3,10] These shortages were driven by the sudden increased demand for RNA extraction kits and for getting them delivered when international transport was becoming an issue.[6,7,8,9]
Although some companies were not seeing any problem [2] others were in greater demand because labs have preferences. Some companies were more popular, or better able to get their robots (which use specific recipes provided by kits sold by the same company) into more labs, than others.

One fallout from this pandemic is that labs may look to more broadly diversify their reliance on any given supplier. And another may that companies developed processes to more quickly surge production capacity including ensuring stocks of key reagents needed in those kits.
But labs can’t just jump ship to another extraction format overnight. Each kit comes from a different company and usually entails changing an established familiar method, or an entire platform (equipment plus kits and plasticware), to something that is new and unfamiliar. Such a change also requires time to ensure the new platform will deliver on what the specific lab needs (size, throughput, turnaround time, speciality, future need) and that its ongoing use won’t, in eth long term, unnecessarily blow out the budget compared other current method.
After this pandemic is finally over, I think we’ll see enhanced lab capacity in labs all over the world. And hopefully a better understanding of how important testing is.
Other lab-related shortages
We’ve also read about shortages of the swabs used to collect specimens from suspected cases [5,11] and of SARS-CoV-2- specific testing kits.[4,11] And of course, shortages of personal protective equipment including gloves.
Within a very short period after the genetic sequence of the SARS-CoV-2 was put online, flexible labs all around the world had designed and ordered their own primers and probes to set up “in-house” tests for SARS-CoV-2. If they didn’t have a virus themselves, then they could optimise their new tests by designing and ordering a piece of the DNA that would span the region that included the primer and probe binding sites. Unfortunately, because of the way companies make their primers and probes and longer DNA strands, this resulted in at least some having their primer and probe manufacturing processes contaminated by those “synthetic” controls.[12,13]
Summary
So hopefully this explains how kits, reagents and viruses fit together and adds some context for what was happening around their use, and shortages, early on in the pandemic. If not – ask me a question below and I’ll add more info into this post.
References
- The Protein Data Bank H.M. Berman, J. Westbrook, Z. Feng, G. Gilliland, T.N. Bhat, H. Weissig, I.N. Shindyalov, P.E. Bourne (2000) Nucleic Acids Research, 28: 235-242. doi:10.1093/nar/28.1.235
- Availability of RNA Isolation Kits Not as Dire as Reported https://www.biocompare.com/Life-Science-News/561924-Availability-of-RNA-Isolation-Kits-Not-as-Dire-as-Reported/
- Global shortage of Covid-19 test kits hits Australia as other nations limit exports https://www.theguardian.com/australia-news/2020/mar/13/global-shortage-of-covid-19-test-kits-hits-australia-as-other-nations-limit-exports
- Shortage of kits delays labs from testing Covid-19 https://economictimes.indiatimes.com/news/politics-and-nation/shortage-of-kits-delays-labs-from-testing-covid-19/articleshow/74858534.cms?from=mdr
- US virus testing faces new headwind: Lab supply shortages https://abcnews.go.com/Health/wireStory/us-virus-testing-faces-headwind-lab-supply-shortages-69710161
- Shortage of RNA extraction kits hampers efforts to ramp up COVID-19 coronavirus testing https://cen.acs.org/analytical-chemistry/diagnostics/Shortage-RNA-extraction-kits-hampers/98/web/2020/03
- QIAGEN dramatically ramping up global production capacity for RNA extraction kits for use in detection of SARS-CoV-2 coronavirus https://corporate.qiagen.com/newsroom/press-releases/2020/20200317_capacity_increase
- Supply chain issues hit testing ramp-up: Roche Diagnostics India MD Shravan Subramanyam https://economictimes.indiatimes.com/industry/healthcare/biotech/healthcare/supply-chain-issues-hit-testing-ramp-up-roche-diagnostics-india-md-shravan-subramanyam/articleshow/75076431.cms
- Shortage of crucial chemicals creates new obstacle to U.S. coronavirus testing https://www.statnews.com/2020/03/10/shortage-crucial-chemicals-us-coronavirus-testing/comment-page-1/
- Here are the coronavirus testing materials that are in short supply in the US https://qz.com/1822596/all-the-coronavirus-test-materials-in-short-supply-in-the-us/
- Severe shortages of swabs and other supplies hamper coronavirus testing https://edition.cnn.com/2020/03/18/us/coronovirus-testing-supply-shortages-invs/index.html
- Coronavirus Testing Kits Heading To UK Contaminated With COVID-19 https://travelnoire.com/coronavirus-testing-kits-contaminated
- Coronavirus testing effort hampered by kits contaminated with Covid-19 https://www.telegraph.co.uk/news/2020/03/30/uks-attempt-ramp-coronavirus-testing-hindered-key-components/
- Shortage of RNA extraction kits threatens coronavirus testing https://www.scienceboard.net/index.aspx?sec=sup&sub=gen&pag=dis&ItemID=564
International
Copper Soars, Iron Ore Tumbles As Goldman Says “Copper’s Time Is Now”
Copper Soars, Iron Ore Tumbles As Goldman Says "Copper’s Time Is Now"
After languishing for the past two years in a tight range despite recurring…
Share this:


After languishing for the past two years in a tight range despite recurring speculation about declining global supply, copper has finally broken out, surging to the highest price in the past year, just shy of $9,000 a ton as supply cuts hit the market; At the same time the price of the world's "other" most important mined commodity has diverged, as iron ore has tumbled amid growing demand headwinds out of China's comatose housing sector where not even ghost cities are being built any more.
Copper surged almost 5% this week, ending a months-long spell of inertia, as investors focused on risks to supply at various global mines and smelters. As Bloomberg adds, traders also warmed to the idea that the worst of a global downturn is in the past, particularly for metals like copper that are increasingly used in electric vehicles and renewables.
Yet the commodity crash of recent years is hardly over, as signs of the headwinds in traditional industrial sectors are still all too obvious in the iron ore market, where futures fell below $100 a ton for the first time in seven months on Friday as investors bet that China’s years-long property crisis will run through 2024, keeping a lid on demand.

Indeed, while the mood surrounding copper has turned almost euphoric, sentiment on iron ore has soured since the conclusion of the latest National People’s Congress in Beijing, where the CCP set a 5% goal for economic growth, but offered few new measures that would boost infrastructure or other construction-intensive sectors.
As a result, the main steelmaking ingredient has shed more than 30% since early January as hopes of a meaningful revival in construction activity faded. Loss-making steel mills are buying less ore, and stockpiles are piling up at Chinese ports. The latest drop will embolden those who believe that the effects of President Xi Jinping’s property crackdown still have significant room to run, and that last year’s rally in iron ore may have been a false dawn.
Meanwhile, as Bloomberg notes, on Friday there were fresh signs that weakness in China’s industrial economy is hitting the copper market too, with stockpiles tracked by the Shanghai Futures Exchange surging to the highest level since the early days of the pandemic. The hope is that headwinds in traditional industrial areas will be offset by an ongoing surge in usage in electric vehicles and renewables.
And while industrial conditions in Europe and the US also look soft, there’s growing optimism about copper usage in India, where rising investment has helped fuel blowout growth rates of more than 8% — making it the fastest-growing major economy.
In any case, with the demand side of the equation still questionable, the main catalyst behind copper’s powerful rally is an unexpected tightening in global mine supplies, driven mainly by last year’s closure of a giant mine in Panama (discussed here), but there are also growing worries about output in Zambia, which is facing an El Niño-induced power crisis.
On Wednesday, copper prices jumped on huge volumes after smelters in China held a crisis meeting on how to cope with a sharp drop in processing fees following disruptions to supplies of mined ore. The group stopped short of coordinated production cuts, but pledged to re-arrange maintenance work, reduce runs and delay the startup of new projects. In the coming weeks investors will be watching Shanghai exchange inventories closely to gauge both the strength of demand and the extent of any capacity curtailments.
“The increase in SHFE stockpiles has been bigger than we’d anticipated, but we expect to see them coming down over the next few weeks,” Colin Hamilton, managing director for commodities research at BMO Capital Markets, said by phone. “If the pace of the inventory builds doesn’t start to slow, investors will start to question whether smelters are actually cutting and whether the impact of weak construction activity is starting to weigh more heavily on the market.”
* * *
Few have been as happy with the recent surge in copper prices as Goldman's commodity team, where copper has long been a preferred trade (even if it may have cost the former team head Jeff Currie his job due to his unbridled enthusiasm for copper in the past two years which saw many hedge fund clients suffer major losses).
As Goldman's Nicholas Snowdon writes in a note titled "Copper's time is now" (available to pro subscribers in the usual place)...

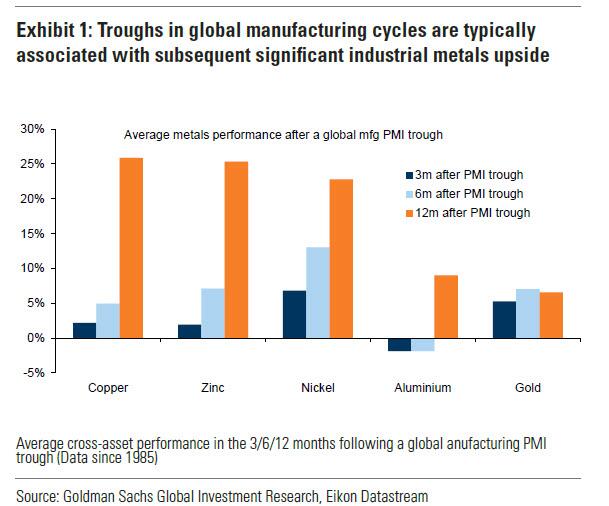
... there has been a "turn in the industrial cycle." Specifically according to the Goldman analyst, after a prolonged downturn, "incremental evidence now points to a bottoming out in the industrial cycle, with the global manufacturing PMI in expansion for the first time since September 2022." As a result, Goldman now expects copper to rise to $10,000/t by year-end and then $12,000/t by end of Q1-25.’
Here are the details:
Previous inflexions in global manufacturing cycles have been associated with subsequent sustained industrial metals upside, with copper and aluminium rising on average 25% and 9% over the next 12 months. Whilst seasonal surpluses have so far limited a tightening alignment at a micro level, we expect deficit inflexions to play out from quarter end, particularly for metals with severe supply binds. Supplemented by the influence of anticipated Fed easing ahead in a non-recessionary growth setting, another historically positive performance factor for metals, this should support further upside ahead with copper the headline act in this regard.
Goldman then turns to what it calls China's "green policy put":
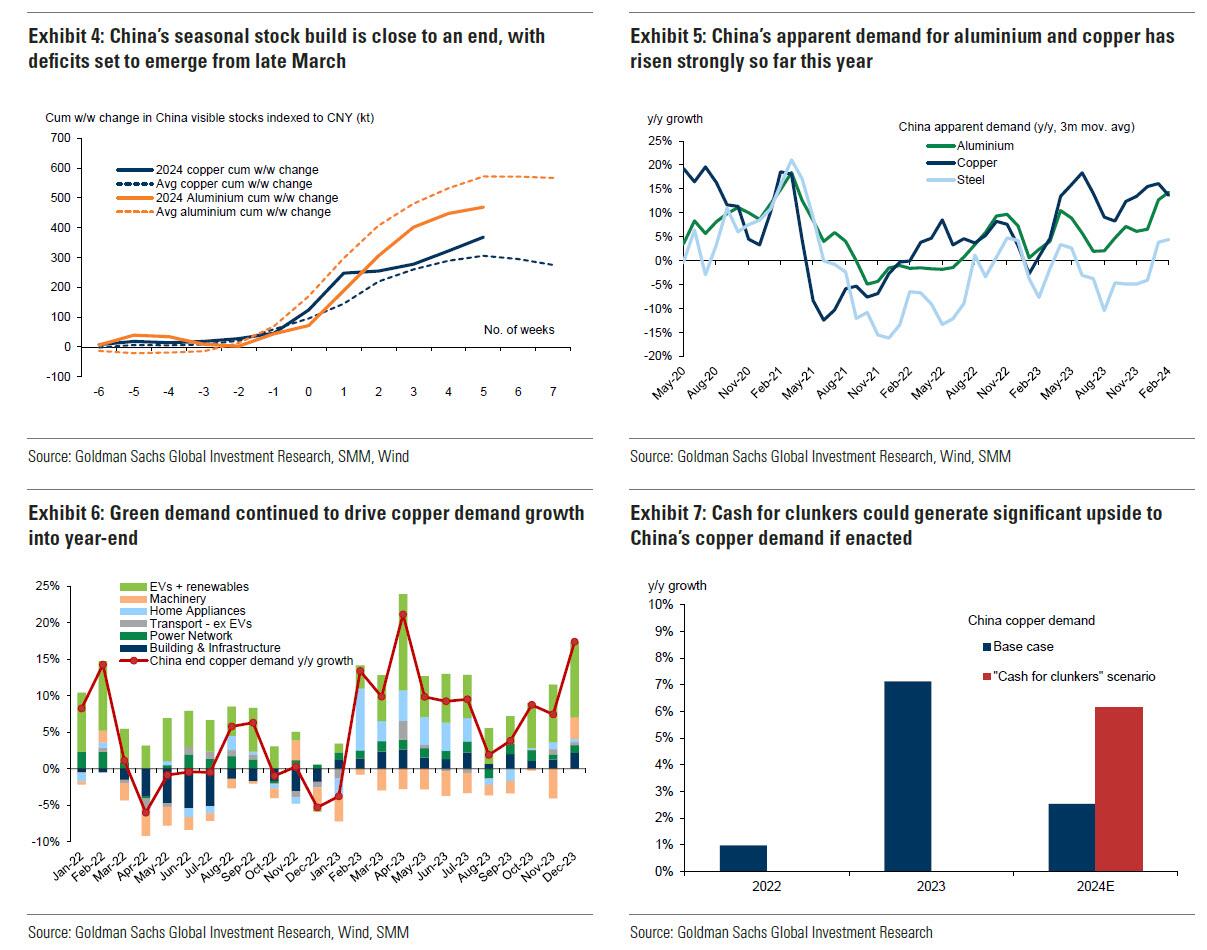
Much of the recent focus on the “Two Sessions” event centred on the lack of significant broad stimulus, and in particular the limited property support. In our view it would be wrong – just as in 2022 and 2023 – to assume that this will result in weak onshore metals demand. Beijing’s emphasis on rapid growth in the metals intensive green economy, as an offset to property declines, continues to act as a policy put for green metals demand. After last year’s strong trends, evidence year-to-date is again supportive with aluminium and copper apparent demand rising 17% and 12% y/y respectively. Moreover, the potential for a ‘cash for clunkers’ initiative could provide meaningful right tail risk to that healthy demand base case. Yet there are also clear metal losers in this divergent policy setting, with ongoing pressure on property related steel demand generating recent sharp iron ore downside.
Meanwhile, Snowdon believes that the driver behind Goldman's long-running bullish view on copper - a global supply shock - continues:
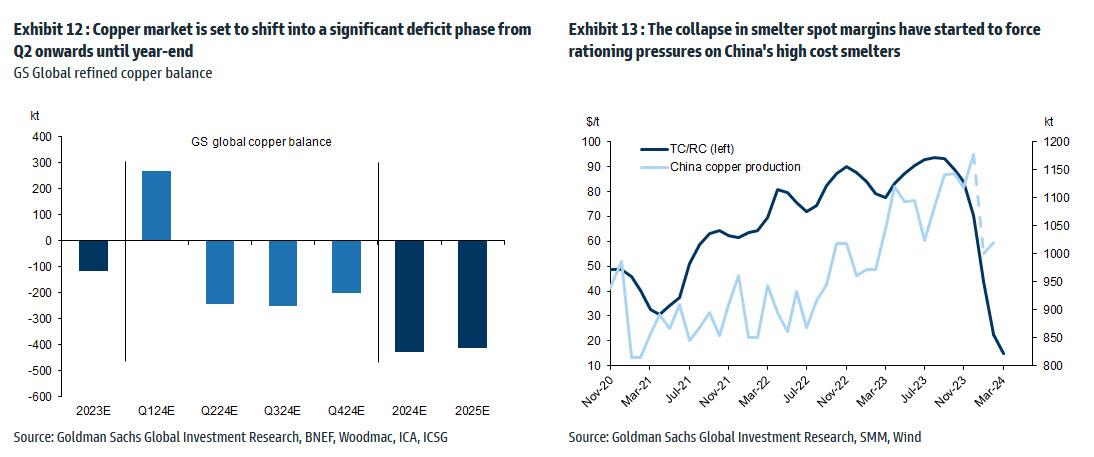
Copper’s supply shock progresses. The metal with most significant upside potential is copper, in our view. The supply shock which began with aggressive concentrate destocking and then sharp mine supply downgrades last year, has now advanced to an increasing bind on metal production, as reflected in this week's China smelter supply rationing signal. With continued positive momentum in China's copper demand, a healthy refined import trend should generate a substantial ex-China refined deficit this year. With LME stocks having halved from Q4 peak, China’s imminent seasonal demand inflection should accelerate a path into extreme tightness by H2. Structural supply underinvestment, best reflected in peak mine supply we expect next year, implies that demand destruction will need to be the persistent solver on scarcity, an effect requiring substantially higher pricing than current, in our view. In this context, we maintain our view that the copper price will surge into next year (GSe 2025 $15,000/t average), expecting copper to rise to $10,000/t by year-end and then $12,000/t by end of Q1-25’
Another reason why Goldman is doubling down on its bullish copper outlook: gold.
The sharp rally in gold price since the beginning of March has ended the period of consolidation that had been present since late December. Whilst the initial catalyst for the break higher came from a (gold) supportive turn in US data and real rates, the move has been significantly amplified by short term systematic buying, which suggests less sticky upside. In this context, we expect gold to consolidate for now, with our economists near term view on rates and the dollar suggesting limited near-term catalysts for further upside momentum. Yet, a substantive retracement lower will also likely be limited by resilience in physical buying channels. Nonetheless, in the midterm we continue to hold a constructive view on gold underpinned by persistent strength in EM demand as well as eventual Fed easing, which should crucially reactivate the largely for now dormant ETF buying channel. In this context, we increase our average gold price forecast for 2024 from $2,090/toz to $2,180/toz, targeting a move to $2,300/toz by year-end.
Much more in the full Goldman note available to pro subs.
International
The millions of people not looking for work in the UK may be prioritising education, health and freedom
Economic inactivity is not always the worst option.
Share this:


Around one in five British people of working age (16-64) are now outside the labour market. Neither in work nor looking for work, they are officially labelled as “economically inactive”.
Some of those 9.2 million people are in education, with many students not active in the labour market because they are studying full-time. Others are older workers who have chosen to take early retirement.
But that still leaves a large number who are not part of the labour market because they are unable to work. And one key driver of economic inactivity in recent years has been illness.
This increase in economic inactivity – which has grown since before the pandemic – is not just harming the economy, but also indicative of a deeper health crisis.
For those suffering ill health, there are real constraints on access to work. People with health-limiting conditions cannot just slot into jobs that are available. They need help to address the illnesses they have, and to re-engage with work through organisations offering supportive and healthy work environments.
And for other groups, such as stay-at-home parents, businesses need to offer flexible work arrangements and subsidised childcare to support the transition from economic inactivity into work.
The government has a role to play too. Most obviously, it could increase investment in the NHS. Rising levels of poor health are linked to years of under-investment in the health sector and economic inactivity will not be tackled without more funding.
Carrots and sticks
For the time being though, the UK government appears to prefer an approach which mixes carrots and sticks. In the March 2024 budget, for example, the chancellor cut national insurance by 2p as a way of “making work pay”.
But it is unclear whether small tax changes like this will have any effect on attracting the economically inactive back into work.
Jeremy Hunt also extended free childcare. But again, questions remain over whether this is sufficient to remove barriers to work for those with parental responsibilities. The high cost and lack of availability of childcare remain key weaknesses in the UK economy.
The benefit system meanwhile has been designed to push people into work. Benefits in the UK remain relatively ungenerous and hard to access compared with other rich countries. But labour shortages won’t be solved by simply forcing the economically inactive into work, because not all of them are ready or able to comply.
It is also worth noting that work itself may be a cause of bad health. The notion of “bad work” – work that does not pay enough and is unrewarding in other ways – can lead to economic inactivity.
There is also evidence that as work has become more intensive over recent decades, for some people, work itself has become a health risk.
The pandemic showed us how certain groups of workers (including so-called “essential workers”) suffered more ill health due to their greater exposure to COVID. But there are broader trends towards lower quality work that predate the pandemic, and these trends suggest improving job quality is an important step towards tackling the underlying causes of economic inactivity.
Freedom
Another big section of the economically active population who cannot be ignored are those who have retired early and deliberately left the labour market behind. These are people who want and value – and crucially, can afford – a life without work.
Here, the effects of the pandemic can be seen again. During those years of lockdowns, furlough and remote working, many of us reassessed our relationship with our jobs. Changed attitudes towards work among some (mostly older) workers can explain why they are no longer in the labour market and why they may be unresponsive to job offers of any kind.

And maybe it is from this viewpoint that we should ultimately be looking at economic inactivity – that it is actually a sign of progress. That it represents a move towards freedom from the drudgery of work and the ability of some people to live as they wish.
There are utopian visions of the future, for example, which suggest that individual and collective freedom could be dramatically increased by paying people a universal basic income.
In the meantime, for plenty of working age people, economic inactivity is a direct result of ill health and sickness. So it may be that the levels of economic inactivity right now merely show how far we are from being a society which actually supports its citizens’ wellbeing.
David Spencer has received funding from the ESRC.
uk pandemicInternational
Illegal Immigrants Leave US Hospitals With Billions In Unpaid Bills
Illegal Immigrants Leave US Hospitals With Billions In Unpaid Bills
By Autumn Spredemann of The Epoch Times
Tens of thousands of illegal…
Share this:

{kind=link}

By Autumn Spredemann of The Epoch Times
Tens of thousands of illegal immigrants are flooding into U.S. hospitals for treatment and leaving billions in uncompensated health care costs in their wake.
{kind=link}
The House Committee on Homeland Security recently released a report illustrating that from the estimated $451 billion in annual costs stemming from the U.S. border crisis, a significant portion is going to health care for illegal immigrants.
With the majority of the illegal immigrant population lacking any kind of medical insurance, hospitals and government welfare programs such as Medicaid are feeling the weight of these unanticipated costs.
Apprehensions of illegal immigrants at the U.S. border have jumped 48 percent since the record in fiscal year 2021 and nearly tripled since fiscal year 2019, according to Customs and Border Protection data.
Last year broke a new record high for illegal border crossings, surpassing more than 3.2 million apprehensions.
And with that sea of humanity comes the need for health care and, in most cases, the inability to pay for it.
In January, CEO of Denver Health Donna Lynne told reporters that 8,000 illegal immigrants made roughly 20,000 visits to the city’s health system in 2023.
The total bill for uncompensated care costs last year to the system totaled $140 million, said Dane Roper, public information officer for Denver Health. More than $10 million of it was attributed to “care for new immigrants,” he told The Epoch Times.
Though the amount of debt assigned to illegal immigrants is a fraction of the total, uncompensated care costs in the Denver Health system have risen dramatically over the past few years.
The total uncompensated costs in 2020 came to $60 million, Mr. Roper said. In 2022, the number doubled, hitting $120 million.
He also said their city hospitals are treating issues such as “respiratory illnesses, GI [gastro-intenstinal] illnesses, dental disease, and some common chronic illnesses such as asthma and diabetes.”
“The perspective we’ve been trying to emphasize all along is that providing healthcare services for an influx of new immigrants who are unable to pay for their care is adding additional strain to an already significant uncompensated care burden,” Mr. Roper said.
He added this is why a local, state, and federal response to the needs of the new illegal immigrant population is “so important.”
Colorado is far from the only state struggling with a trail of unpaid hospital bills.

Dr. Robert Trenschel, CEO of the Yuma Regional Medical Center situated on the Arizona–Mexico border, said on average, illegal immigrants cost up to three times more in human resources to resolve their cases and provide a safe discharge.
“Some [illegal] migrants come with minor ailments, but many of them come in with significant disease,” Dr. Trenschel said during a congressional hearing last year.
“We’ve had migrant patients on dialysis, cardiac catheterization, and in need of heart surgery. Many are very sick.”
He said many illegal immigrants who enter the country and need medical assistance end up staying in the ICU ward for 60 days or more.
A large portion of the patients are pregnant women who’ve had little to no prenatal treatment. This has resulted in an increase in babies being born that require neonatal care for 30 days or longer.
Dr. Trenschel told The Epoch Times last year that illegal immigrants were overrunning healthcare services in his town, leaving the hospital with $26 million in unpaid medical bills in just 12 months.
ER Duty to Care
The Emergency Medical Treatment and Labor Act of 1986 requires that public hospitals participating in Medicare “must medically screen all persons seeking emergency care … regardless of payment method or insurance status.”
The numbers are difficult to gauge as the policy position of the Centers for Medicare & Medicaid Services (CMS) is that it “will not require hospital staff to ask patients directly about their citizenship or immigration status.”
In southern California, again close to the border with Mexico, some hospitals are struggling with an influx of illegal immigrants.
American patients are enduring longer wait times for doctor appointments due to a nursing shortage in the state, two health care professionals told The Epoch Times in January.
A health care worker at a hospital in Southern California, who asked not to be named for fear of losing her job, told The Epoch Times that “the entire health care system is just being bombarded” by a steady stream of illegal immigrants.
“Our healthcare system is so overwhelmed, and then add on top of that tuberculosis, COVID-19, and other diseases from all over the world,” she said.

A newly-enacted law in California provides free healthcare for all illegal immigrants residing in the state. The law could cost taxpayers between $3 billion and $6 billion per year, according to recent estimates by state and federal lawmakers.
In New York, where the illegal immigration crisis has manifested most notably beyond the southern border, city and state officials have long been accommodating of illegal immigrants’ healthcare costs.
Since June 2014, when then-mayor Bill de Blasio set up The Task Force on Immigrant Health Care Access, New York City has worked to expand avenues for illegal immigrants to get free health care.
“New York City has a moral duty to ensure that all its residents have meaningful access to needed health care, regardless of their immigration status or ability to pay,” Mr. de Blasio stated in a 2015 report.
The report notes that in 2013, nearly 64 percent of illegal immigrants were uninsured. Since then, tens of thousands of illegal immigrants have settled in the city.
“The uninsured rate for undocumented immigrants is more than three times that of other noncitizens in New York City (20 percent) and more than six times greater than the uninsured rate for the rest of the city (10 percent),” the report states.
The report states that because healthcare providers don’t ask patients about documentation status, the task force lacks “data specific to undocumented patients.”
Some health care providers say a big part of the issue is that without a clear path to insurance or payment for non-emergency services, illegal immigrants are going to the hospital due to a lack of options.
“It’s insane, and it has been for years at this point,” Dana, a Texas emergency room nurse who asked to have her full name omitted, told The Epoch Times.
Working for a major hospital system in the greater Houston area, Dana has seen “a zillion” migrants pass through under her watch with “no end in sight.” She said many who are illegal immigrants arrive with treatable illnesses that require simple antibiotics. “Not a lot of GPs [general practitioners] will see you if you can’t pay and don’t have insurance.”
She said the “undocumented crowd” tends to arrive with a lot of the same conditions. Many find their way to Houston not long after crossing the southern border. Some of the common health issues Dana encounters include dehydration, unhealed fractures, respiratory illnesses, stomach ailments, and pregnancy-related concerns.
“This isn’t a new problem, it’s just worse now,” Dana said.

Medicaid Factor
One of the main government healthcare resources illegal immigrants use is Medicaid.
All those who don’t qualify for regular Medicaid are eligible for Emergency Medicaid, regardless of immigration status. By doing this, the program helps pay for the cost of uncompensated care bills at qualifying hospitals.
However, some loopholes allow access to the regular Medicaid benefits. “Qualified noncitizens” who haven’t been granted legal status within five years still qualify if they’re listed as a refugee, an asylum seeker, or a Cuban or Haitian national.
Yet the lion’s share of Medicaid usage by illegal immigrants still comes through state-level benefits and emergency medical treatment.
A Congressional report highlighted data from the CMS, which showed total Medicaid costs for “emergency services for undocumented aliens” in fiscal year 2021 surpassed $7 billion, and totaled more than $5 billion in fiscal 2022.
Both years represent a significant spike from the $3 billion in fiscal 2020.
An employee working with Medicaid who asked to be referred to only as Jennifer out of concern for her job, told The Epoch Times that at a state level, it’s easy for an illegal immigrant to access the program benefits.
Jennifer said that when exceptions are sent from states to CMS for approval, “denial is actually super rare. It’s usually always approved.”
She also said it comes as no surprise that many of the states with the highest amount of Medicaid spending are sanctuary states, which tend to have policies and laws that shield illegal immigrants from federal immigration authorities.
Moreover, Jennifer said there are ways for states to get around CMS guidelines. “It’s not easy, but it can and has been done.”
The first generation of illegal immigrants who arrive to the United States tend to be healthy enough to pass any pre-screenings, but Jennifer has observed that the subsequent generations tend to be sicker and require more access to care. If a family is illegally present, they tend to use Emergency Medicaid or nothing at all.
The Epoch Times asked Medicaid Services to provide the most recent data for the total uncompensated care that hospitals have reported. The agency didn’t respond.
Continue reading over at The Epoch Times


Sylvester researchers, collaborators call for greater investment in bereavement care


Illegal Immigrants Leave US Hospitals With Billions In Unpaid Bills


“I Can’t Even Save”: Americans Are Getting Absolutely Crushed Under Enormous Debt Load


Problems After COVID-19 Vaccination More Prevalent Among Naturally Immune: Study


Looking Back At COVID’s Authoritarian Regimes


Copper Soars, Iron Ore Tumbles As Goldman Says “Copper’s Time Is Now”


Stock Market Today: Stocks turn lower as factory inflation spikes, retail sales miss target


‘Excess Mortality Skyrocketed’: Tucker Carlson and Dr. Pierre Kory Unpack ‘Criminal’ COVID Response


Delta Air Lines adds a new route travelers have been asking for


Separating Information From Disinformation: Threats From The AI Revolution
-

 Uncategorized3 weeks ago
Uncategorized3 weeks agoAll Of The Elements Are In Place For An Economic Crisis Of Staggering Proportions
-

 International1 week ago
International1 week agoEyePoint poaches medical chief from Apellis; Sandoz CFO, longtime BioNTech exec to retire
-

 Uncategorized4 weeks ago
Uncategorized4 weeks agoCalifornia Counties Could Be Forced To Pay $300 Million To Cover COVID-Era Program
-

 Uncategorized3 weeks ago
Uncategorized3 weeks agoApparel Retailer Express Moving Toward Bankruptcy
-

 Uncategorized4 weeks ago
Uncategorized4 weeks agoIndustrial Production Decreased 0.1% in January
-

 International1 week ago
International1 week agoWalmart launches clever answer to Target’s new membership program
-

 Spread & Containment3 days ago
Spread & Containment3 days agoIFM’s Hat Trick and Reflections On Option-To-Buy M&A
-

 Uncategorized4 weeks ago
Uncategorized4 weeks agoRFK Jr: The Wuhan Cover-Up & The Rise Of The Biowarfare-Industrial Complex