International
The Next Step For The World Economic Forum
The Next Step For The World Economic Forum
Authored by Roger Koops via The Brownstone Institute,
It has been obvious since early 2020 that…
Share this:


Authored by Roger Koops via The Brownstone Institute,
It has been obvious since early 2020 that there has been an organized cult outreach that has permeated the world as a whole. It’s possible that this formed out of a gigantic error, rooted in a sudden ignorance of cell biology and long experience of public health. It is also possible that a seasonal respiratory virus was deployed by some people as an opportunity to seize power for some other purpose.
Follow the money and influence trails and the latter conclusion is hard to dismiss.
The clues were there early. Even before the WHO declared a pandemic in March 2020 (at least several months behind the actual fact of a pandemic) and before any lockdowns, there were media blitzes talking about the “New Normal” and talk of the “Great Reset” (which was rebranded as “Build Back Better”).
Pharmaceutical companies such as Pfizer, Johnson & Johnson, Moderna, and Astra-Zeneca were actively lobbying governments to buy their vaccines as early as February 2020, supposedly less than a month after the genetic sequence (or partial sequence) was made available by China.
As a person who spent his whole professional career in pharmaceutical and vaccine development, I found the whole concept of going from scratch to a ready-to-use vaccine in a few months simply preposterous.
Something did not add up.
I knew of the names with which everyone has become familiar. Bill Gates, Neil Ferguson, Jeremy Farrar, Anthony Fauci, and others had either been lobbying for or pursuing the lockdown strategies for many years. But still, the scope of the actions seemed too large to even be explained by those names alone.
So, the fundamental questions that I have been asking myself have been why and who? The “Why” seems to always come back to issues besides public health. Of course the “Who” had the obvious players such as the WHO, China, CDC, NIH/NIAID, and various governments but there seemed to be more behind it than that. These players have been connected to the “public health” aspect but that seemed to be only scratching the surface.
I am not an investigative journalist and I would never claim that role, but even I can do some simple internet searches and start to see patterns evolve. The searches that I have done have yielded some very interesting “coincidences.”
If I give you the names of the following people – Biden, Trudeau, Ardern, Merkel, Macron, Draghi, Morrison, Xi Jinping – what do you think that they have in common? Yes, they are all pampered and stumble over themselves, but that is also not the connection.
One can see very quickly that these names certainly connect to lockdown countries and individuals who have ignored their own laws and/or tried in some way to usurp them. But, there is more to it than that and I will give a hint by providing a link with each name.
-
Joseph Biden, President, United States
-
Boris Johnson, PM of United Kingdom
-
Jacinda Ardern, PM of New Zealand
-
Angela Merkel, Former PM of Germany
-
Emmanuel Macron, President of France
-
Justin Trudeau, PM of Canada
-
Xi Jinping, CCP Leader, China
-
Mario Draghi, PM of Italy
-
Scott Morrison, PM of Australia
They are all associated with the World Economic Forum (WEF), a “nonprofit” private organization started (in 1971) and headed by Klaus “You will own nothing and be happy” Schwab and his family. This is a private organization that has no official bearing with any world governance body, despite the implication of the name. It could just as well have been called the “Church of Schwabies.” The WEF was the origin of the “Great Reset” and I would guess that it was the origin of “Build Back Better” (since most of the above names have used that term recently).
If you think that the WEF membership ends with just leaders of countries, here are a few more names:
-
Gavin Newsom, Governor of California
-
Jay Inslee, Governor of Washington State
-
Anthony Fauci, Director NIAID
-
Nancy Pelosi, Speaker of the House
Allow me to introduce more of the WEF by giving a list of names for the Board of Trustees.
-
Al Gore, Former WP of the US
-
Mark Caney, UN Special Envoy for Climate Action
-
T. Shanmugaratnam, Seminar Minister Singapore
-
Christine Lagarde, President, European Central Bank
-
Ngozi Okonja-Iweala, Director General, WTO
-
Kristalian Georggieva, Managing Director, IMF
-
Chrystia Freeland, Deputy Minister of Canada
-
Laurence Fink, CEO, BlackRock
You can see a cross section of political and economic leaders on the board. The leader of the organization, that is the leader of the Board, is still Klaus Schwab. He has built an impressive array of followers.
If you want to really see the extent of influence, go to the website and pick out the corporate name of your choice; there are many to choose from: Abbott Laboratories, Astra-Zeneca, Biogen, Johnson & Johnson, Moderna, Merck, Novartis, Pfizer, Serum Institute of India, BASF, Mayo Clinic, Kaiser Permanente, Bill and Melinda Gates Foundation, Wellcome Trust, Blackrock, CISCO, Dell, Google, Huawei, IBM, Intel, Microsoft, Zoom, Yahoo, Amazon, Airbus, Boeing, Honda, Rakuten, Walmart, UPS, Coca-Cola, UBER, Bank of China. Bank of America. Deutsche Bank, State Bank of India, Royal Bank of Canada, Lloyds Banking, JP Morgan-Chase, Equifax, Goldman-Sachs, Hong Kong Exchanges, Bloomberg, VISA, New York Times, Ontario (Canada) Teacher’s Pension Plan
The extent of reach is huge even beyond the worldwide leader network. For example, we all know what Bill Gates has been doing with his wealth via the Bill and Melinda Gates Foundation (BMGF). But, the Wellcome Trust is equal to the task. Who is the Director of the Wellcome Trust? One named Jeremy Farrar, of the United Kingdom SAGE and lockdown fame – arguably the architect of the US-UK lockdowns in 2020 – is closely associated with WEF.
Concerning the reach that can occur, let me give some examples from the BMGF alone, and it comes from the time that I spent in 2020 reading their extensive funding list.
A few years ago, the BMGF awarded the Institute for Health Metric Evaluation (IHME) a ten-year, almost $280 million award. IHME (associated with the University of Washington in Seattle) was at the forefront of the computer modeling that was driving the lockdowns and the nonpharmaceutical Interventions during 2020. People have seen their name often in print or on MSNBC or CNN.
In 2019, IHME awarded the Editor of the Lancet (Dr. Richard Horton) a $100,000 award and described him as an “activist editor.” The Lancet, once considered one of the best medical journals, has been at the forefront of censoring opposing scientific viewpoints since 2020 and publishing “papers” that were not fit to be published. I never could understand what it meant to be an “activist” editor in a respected scientific/medical journal because, stupid me, I always thought that the first job of the editor was to be impartial. I guess I learned in 2020 how wrong I was.
Of course, the Lancet is also heavily funded from pharmaceutical companies such as Pfizer (also a member of the WEF).
But, the BMGF reach goes far beyond just IHME and these connections have been quite recognizable. Here are some examples of the organizations and moneys received during 2020 alone broken down by areas.
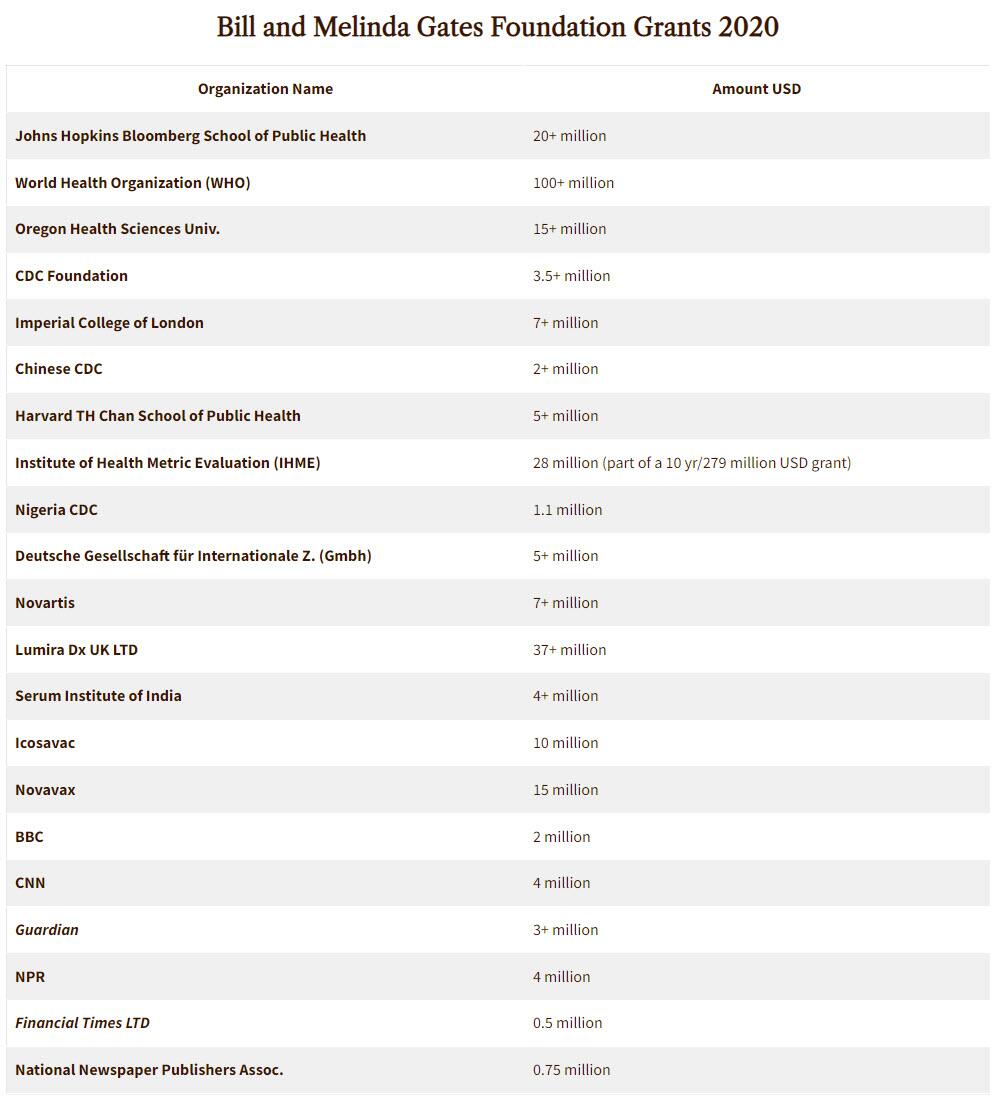
Bill Gates has also invested heavily in Moderna and his investments have paid out nicely for him. The BMGF has also given close to $100 million to the Clinton Health Access Initiative.
The questions now have to be asked:
-
Is this some beginning of a controlled authoritarian society intertwined via the WEF?
-
Has the Covid panic been staged to set the stage? Please note, I am not a “Covid Denier” since the virus is real. But, has a normal seasonal respiratory virus been used as an excuse to activate the web?
The next questions, for those of us who at least pretend to live in “Democratic” societies, have to be:
-
Is this what you expected and/or want from the people you elect?
-
How many people knew of the “Associations” of the people that they voted for? (I certainly did not know of the associations until I did the searches but maybe I am just out of touch)
Can we anticipate their next moves? There may be some hints.
The Next Move
Jeremy Farrar of The Wellcome Trust recently wrote an article for the WEF with the CEO of Novo Nordisk Foundation, Mads Krogsgaard Thomsen. It is a summary of a larger piece written for and published by the Boston Consulting Group.
In this article, they propose that the way to “fix” the problem of antibiotic resistant bacteria is via a subscription service. That is, you pay a fee and when you need an antibiotic, presumably an effective one will be available for you.
My guess is that they have the same philosophy for vaccines and that certainly seems to be the approach with Coronavirus. Keep paying for and taking boosters.
In view of this philosophy, the vaccine mandates make sense. Get society “addicted” to an intervention, effective or not, and then keep feeding them. This becomes especially effective if you can keep the fear going.
This approach is so shortsighted, from a scientific viewpoint, it astounds me. But, like much of recent history, I think science has little to do with it. The goal is not scientifically founded but control founded.
After the discovery of penicillin almost one century ago, there were scientists who warned that antibiotic usage should be considered very carefully in practice because evolutionary pressures would lead to antibiotic resistant species of bacteria. At that time, they were considered to be rogue scientists; after all, didn’t we suddenly have a miracle cure for many deadly problems?
From the time of discovery, it took over a decade before fermentation methods were developed to produce sufficient quantities of antibiotics to be practical. These methods allowed for the use of penicillin on the battlefield towards the end of WWII and undoubtedly saved many lives then and later in subsequent wars (Korea and Vietnam) by preventing serious infections resulting from wounds sustained during battle.
However, it did not take long before the medical establishment was handing out antibiotics like candy. I experienced this myself when I was a child in the 1960s. It seemed like every time we went to the doctor, no matter what the problem, I was given a series (not just one) of injections of penicillin. There were never any attempts to determine if I had a virus, bacteria, or even an allergy. The answer was: in with the needle. I cannot count how many times I was “jabbed” as a child.
It didn’t take long before resistance species started to appear. The result was that more and more money was pumped into R&D for antibiotics. When I was in graduate school during the 1980s, one sure way to get some NIH funding was to tie the research into the “antibiotic” search. Antibiotics became big business.
We now have several classes of antibiotics that are used for specific cases. We have Aminoglycosides (Streptomycin, Neomycin, etc.), Beta-Lactams Cephalosporins (four generations including Cefadroxil-G1, Cefaclor-G2, Cefotaxime-G3, Cefepime-G4 , Beta-Lactams Penicillins (including Ampicillin, Amoxicillin, and Penicillin), Other Beta-Lactams (Meropenem), Fluoroquinolones (Levofloxacin, Gemifloxicin, etc.), Macrolides (Azithromycin, Clarithromycin, etc.), Sulfonamides (Sulfisoxazole, etc.), Tetracyclines, and others such as Clindamycin and Vancomycin (typically reserved for resistant bacteria). All in all, physicians have over 50 different choices for antibiotics.
The most common place to encounter antibiotic resistant bacteria is in a hospital. Most people who get some sort of infection in the normal routine of life, like a sinus infection or skin infection, will not likely encounter an antibiotic resistant species.
Except there has been another source of the problem and that has been in the food supply. Antibiotics have become very popular with large scale meat production facilities of all types including beef, poultry, swine, and even fish. These include actual farms where the animals are raised as well as in the processing of the meat. The overuse of antibiotics in these industries has also produced resistant forms of bacteria.
For example, in attempts to limit the bacteria e. coli, common to mammalians, antibiotics have been used and this has resulted in some antibiotic resistant forms of e. coli. An infection via e. coli (antibiotic resistant or not) can be avoided by proper cooking and handling of meats. However, sometimes that does not happen and there are e. coli outbreaks (also from improperly washed vegetables that may use contaminated irrigation water).
For most healthy people, experiencing e. coli (either resistant or not) is only a passing discomfort that includes intestinal cramps, diarrhea, and other GI complaints. Depending on the amount of contamination, a person may suffer for a day or two or for several days.
But, with some people, it can be serious or deadly (such as in elderly people in poor health and young children). If that occurs, then the presence of an antibiotic resistant form can be a serious matter. Presence of a non-resistant form can be treated more readily.
A few years ago I had pneumonia; a relatively mild case. I was given a choice of in-patient treatment or out-patient and it was a no-brainer. If I wanted to make sure that my pneumonia could be handled by the normal course of antibiotics (I was given a quinolone), staying at home and away from the hospital was important. I knew that hospital-acquired pneumonia could be a much more serious situation. So, I stayed at home and easily recovered. That did not mean I was guaranteed getting a more serious resistant form in the hospital but I understood that the risk was much greater.
Producing more antibiotics and giving them on subscription to the users is not the answer. That will only lead to more resistant forms and there will be this continuing loop of antibiotic use. But, if the actual goal is societal addiction to antibiotics out of fear, just like addiction to universal Covid vaccines out of fear, then it makes sense.
Finding a few universal antibiotics that deal with the resistant forms is important and it is also important to use those sparingly and only as a last resort. In addition, better management of antibiotic use in our society would go a long way to attenuating the problem.
There is nothing particularly controversial about that observation. It was accepted by nearly every responsible health professional only two years ago. But we live now in different times of extreme experimentation, such as the deployment of world-wide lockdowns for a virus that had a highly focused impact, with catastrophic results for the world.
It was the WEF on March 21, 2020 that assured us “lockdowns can halt the spread of Covid-19.” Today that article, never pulled much less repudiated, stands as probably the most ridiculous and destructive suggestion and prediction of the 21st century. And yet, the WEF is still at it, suggesting that same year that at least lockdowns reduced carbon emissions.
We can easily predict that the WEF’s call for a universal and mandated subscription plan for antibiotics – pushed with the overt intention of shoring up financial capitalization of major drug manufacturers – will meet the same fate: poor health outcomes, more power to entrenched elites, and ever less liberty for the people.
International
Copper Soars, Iron Ore Tumbles As Goldman Says “Copper’s Time Is Now”
Copper Soars, Iron Ore Tumbles As Goldman Says "Copper’s Time Is Now"
After languishing for the past two years in a tight range despite recurring…
Share this:


After languishing for the past two years in a tight range despite recurring speculation about declining global supply, copper has finally broken out, surging to the highest price in the past year, just shy of $9,000 a ton as supply cuts hit the market; At the same time the price of the world's "other" most important mined commodity has diverged, as iron ore has tumbled amid growing demand headwinds out of China's comatose housing sector where not even ghost cities are being built any more.
Copper surged almost 5% this week, ending a months-long spell of inertia, as investors focused on risks to supply at various global mines and smelters. As Bloomberg adds, traders also warmed to the idea that the worst of a global downturn is in the past, particularly for metals like copper that are increasingly used in electric vehicles and renewables.
Yet the commodity crash of recent years is hardly over, as signs of the headwinds in traditional industrial sectors are still all too obvious in the iron ore market, where futures fell below $100 a ton for the first time in seven months on Friday as investors bet that China’s years-long property crisis will run through 2024, keeping a lid on demand.

Indeed, while the mood surrounding copper has turned almost euphoric, sentiment on iron ore has soured since the conclusion of the latest National People’s Congress in Beijing, where the CCP set a 5% goal for economic growth, but offered few new measures that would boost infrastructure or other construction-intensive sectors.
As a result, the main steelmaking ingredient has shed more than 30% since early January as hopes of a meaningful revival in construction activity faded. Loss-making steel mills are buying less ore, and stockpiles are piling up at Chinese ports. The latest drop will embolden those who believe that the effects of President Xi Jinping’s property crackdown still have significant room to run, and that last year’s rally in iron ore may have been a false dawn.
Meanwhile, as Bloomberg notes, on Friday there were fresh signs that weakness in China’s industrial economy is hitting the copper market too, with stockpiles tracked by the Shanghai Futures Exchange surging to the highest level since the early days of the pandemic. The hope is that headwinds in traditional industrial areas will be offset by an ongoing surge in usage in electric vehicles and renewables.
And while industrial conditions in Europe and the US also look soft, there’s growing optimism about copper usage in India, where rising investment has helped fuel blowout growth rates of more than 8% — making it the fastest-growing major economy.
In any case, with the demand side of the equation still questionable, the main catalyst behind copper’s powerful rally is an unexpected tightening in global mine supplies, driven mainly by last year’s closure of a giant mine in Panama (discussed here), but there are also growing worries about output in Zambia, which is facing an El Niño-induced power crisis.
On Wednesday, copper prices jumped on huge volumes after smelters in China held a crisis meeting on how to cope with a sharp drop in processing fees following disruptions to supplies of mined ore. The group stopped short of coordinated production cuts, but pledged to re-arrange maintenance work, reduce runs and delay the startup of new projects. In the coming weeks investors will be watching Shanghai exchange inventories closely to gauge both the strength of demand and the extent of any capacity curtailments.
“The increase in SHFE stockpiles has been bigger than we’d anticipated, but we expect to see them coming down over the next few weeks,” Colin Hamilton, managing director for commodities research at BMO Capital Markets, said by phone. “If the pace of the inventory builds doesn’t start to slow, investors will start to question whether smelters are actually cutting and whether the impact of weak construction activity is starting to weigh more heavily on the market.”
* * *
Few have been as happy with the recent surge in copper prices as Goldman's commodity team, where copper has long been a preferred trade (even if it may have cost the former team head Jeff Currie his job due to his unbridled enthusiasm for copper in the past two years which saw many hedge fund clients suffer major losses).
As Goldman's Nicholas Snowdon writes in a note titled "Copper's time is now" (available to pro subscribers in the usual place)...

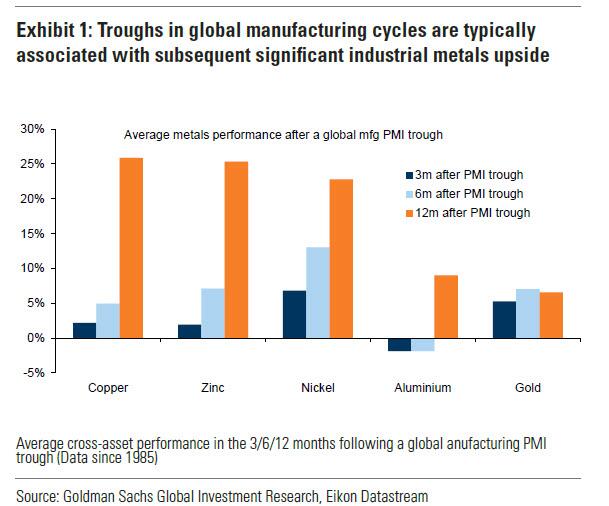
... there has been a "turn in the industrial cycle." Specifically according to the Goldman analyst, after a prolonged downturn, "incremental evidence now points to a bottoming out in the industrial cycle, with the global manufacturing PMI in expansion for the first time since September 2022." As a result, Goldman now expects copper to rise to $10,000/t by year-end and then $12,000/t by end of Q1-25.’
Here are the details:
Previous inflexions in global manufacturing cycles have been associated with subsequent sustained industrial metals upside, with copper and aluminium rising on average 25% and 9% over the next 12 months. Whilst seasonal surpluses have so far limited a tightening alignment at a micro level, we expect deficit inflexions to play out from quarter end, particularly for metals with severe supply binds. Supplemented by the influence of anticipated Fed easing ahead in a non-recessionary growth setting, another historically positive performance factor for metals, this should support further upside ahead with copper the headline act in this regard.
Goldman then turns to what it calls China's "green policy put":
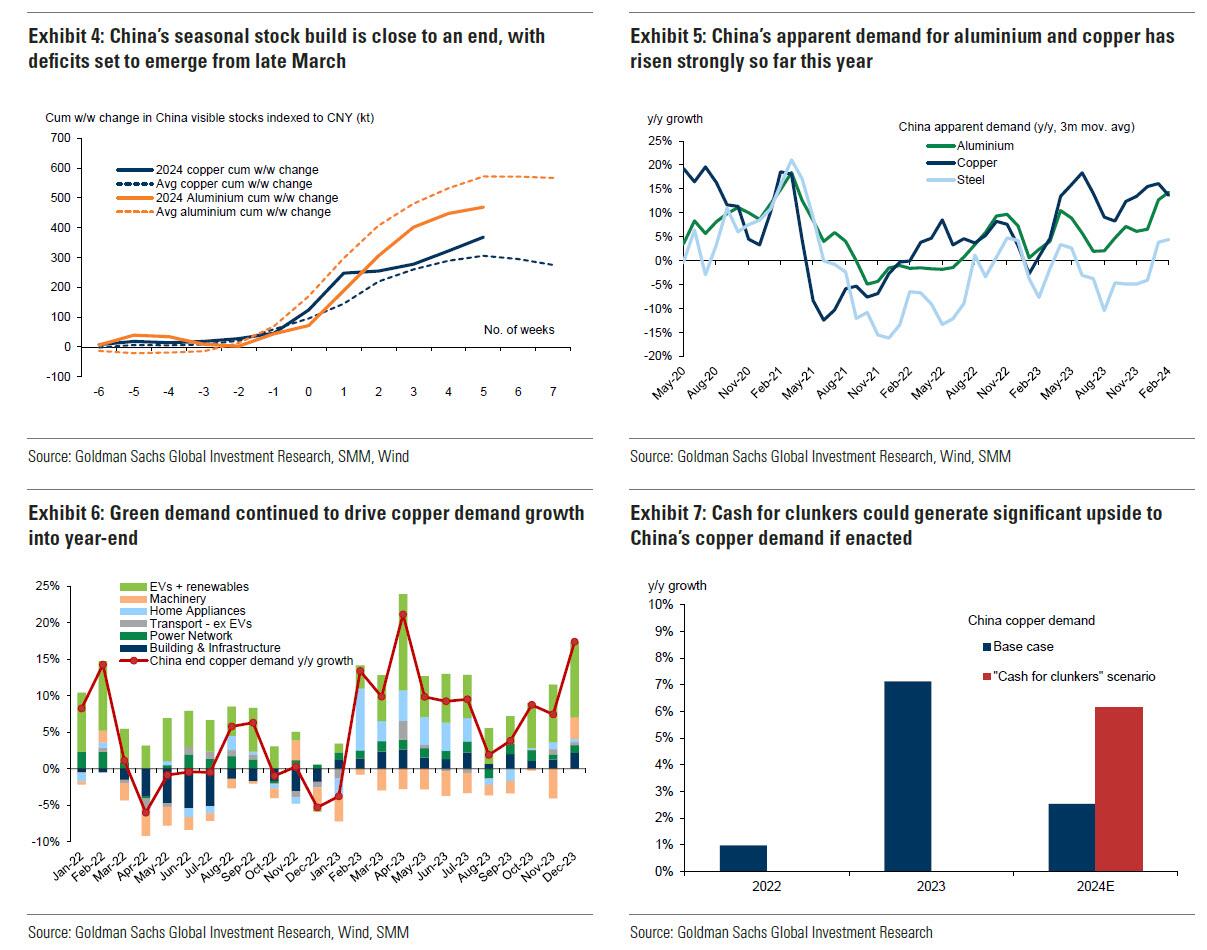
Much of the recent focus on the “Two Sessions” event centred on the lack of significant broad stimulus, and in particular the limited property support. In our view it would be wrong – just as in 2022 and 2023 – to assume that this will result in weak onshore metals demand. Beijing’s emphasis on rapid growth in the metals intensive green economy, as an offset to property declines, continues to act as a policy put for green metals demand. After last year’s strong trends, evidence year-to-date is again supportive with aluminium and copper apparent demand rising 17% and 12% y/y respectively. Moreover, the potential for a ‘cash for clunkers’ initiative could provide meaningful right tail risk to that healthy demand base case. Yet there are also clear metal losers in this divergent policy setting, with ongoing pressure on property related steel demand generating recent sharp iron ore downside.
Meanwhile, Snowdon believes that the driver behind Goldman's long-running bullish view on copper - a global supply shock - continues:
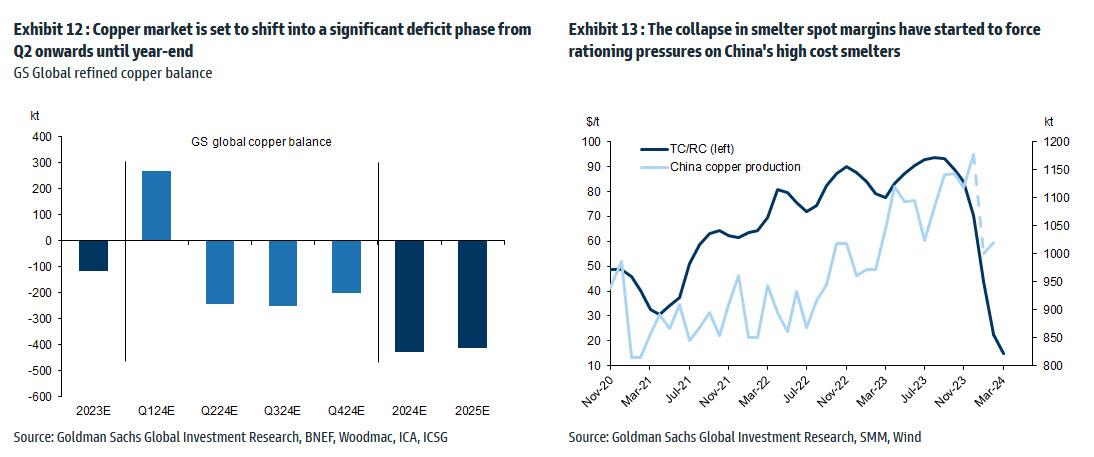
Copper’s supply shock progresses. The metal with most significant upside potential is copper, in our view. The supply shock which began with aggressive concentrate destocking and then sharp mine supply downgrades last year, has now advanced to an increasing bind on metal production, as reflected in this week's China smelter supply rationing signal. With continued positive momentum in China's copper demand, a healthy refined import trend should generate a substantial ex-China refined deficit this year. With LME stocks having halved from Q4 peak, China’s imminent seasonal demand inflection should accelerate a path into extreme tightness by H2. Structural supply underinvestment, best reflected in peak mine supply we expect next year, implies that demand destruction will need to be the persistent solver on scarcity, an effect requiring substantially higher pricing than current, in our view. In this context, we maintain our view that the copper price will surge into next year (GSe 2025 $15,000/t average), expecting copper to rise to $10,000/t by year-end and then $12,000/t by end of Q1-25’
Another reason why Goldman is doubling down on its bullish copper outlook: gold.
The sharp rally in gold price since the beginning of March has ended the period of consolidation that had been present since late December. Whilst the initial catalyst for the break higher came from a (gold) supportive turn in US data and real rates, the move has been significantly amplified by short term systematic buying, which suggests less sticky upside. In this context, we expect gold to consolidate for now, with our economists near term view on rates and the dollar suggesting limited near-term catalysts for further upside momentum. Yet, a substantive retracement lower will also likely be limited by resilience in physical buying channels. Nonetheless, in the midterm we continue to hold a constructive view on gold underpinned by persistent strength in EM demand as well as eventual Fed easing, which should crucially reactivate the largely for now dormant ETF buying channel. In this context, we increase our average gold price forecast for 2024 from $2,090/toz to $2,180/toz, targeting a move to $2,300/toz by year-end.
Much more in the full Goldman note available to pro subs.
International
The millions of people not looking for work in the UK may be prioritising education, health and freedom
Economic inactivity is not always the worst option.
Share this:


Around one in five British people of working age (16-64) are now outside the labour market. Neither in work nor looking for work, they are officially labelled as “economically inactive”.
Some of those 9.2 million people are in education, with many students not active in the labour market because they are studying full-time. Others are older workers who have chosen to take early retirement.
But that still leaves a large number who are not part of the labour market because they are unable to work. And one key driver of economic inactivity in recent years has been illness.
This increase in economic inactivity – which has grown since before the pandemic – is not just harming the economy, but also indicative of a deeper health crisis.
For those suffering ill health, there are real constraints on access to work. People with health-limiting conditions cannot just slot into jobs that are available. They need help to address the illnesses they have, and to re-engage with work through organisations offering supportive and healthy work environments.
And for other groups, such as stay-at-home parents, businesses need to offer flexible work arrangements and subsidised childcare to support the transition from economic inactivity into work.
The government has a role to play too. Most obviously, it could increase investment in the NHS. Rising levels of poor health are linked to years of under-investment in the health sector and economic inactivity will not be tackled without more funding.
Carrots and sticks
For the time being though, the UK government appears to prefer an approach which mixes carrots and sticks. In the March 2024 budget, for example, the chancellor cut national insurance by 2p as a way of “making work pay”.
But it is unclear whether small tax changes like this will have any effect on attracting the economically inactive back into work.
Jeremy Hunt also extended free childcare. But again, questions remain over whether this is sufficient to remove barriers to work for those with parental responsibilities. The high cost and lack of availability of childcare remain key weaknesses in the UK economy.
The benefit system meanwhile has been designed to push people into work. Benefits in the UK remain relatively ungenerous and hard to access compared with other rich countries. But labour shortages won’t be solved by simply forcing the economically inactive into work, because not all of them are ready or able to comply.
It is also worth noting that work itself may be a cause of bad health. The notion of “bad work” – work that does not pay enough and is unrewarding in other ways – can lead to economic inactivity.
There is also evidence that as work has become more intensive over recent decades, for some people, work itself has become a health risk.
The pandemic showed us how certain groups of workers (including so-called “essential workers”) suffered more ill health due to their greater exposure to COVID. But there are broader trends towards lower quality work that predate the pandemic, and these trends suggest improving job quality is an important step towards tackling the underlying causes of economic inactivity.
Freedom
Another big section of the economically active population who cannot be ignored are those who have retired early and deliberately left the labour market behind. These are people who want and value – and crucially, can afford – a life without work.
Here, the effects of the pandemic can be seen again. During those years of lockdowns, furlough and remote working, many of us reassessed our relationship with our jobs. Changed attitudes towards work among some (mostly older) workers can explain why they are no longer in the labour market and why they may be unresponsive to job offers of any kind.

And maybe it is from this viewpoint that we should ultimately be looking at economic inactivity – that it is actually a sign of progress. That it represents a move towards freedom from the drudgery of work and the ability of some people to live as they wish.
There are utopian visions of the future, for example, which suggest that individual and collective freedom could be dramatically increased by paying people a universal basic income.
In the meantime, for plenty of working age people, economic inactivity is a direct result of ill health and sickness. So it may be that the levels of economic inactivity right now merely show how far we are from being a society which actually supports its citizens’ wellbeing.
David Spencer has received funding from the ESRC.
uk pandemicInternational
Illegal Immigrants Leave US Hospitals With Billions In Unpaid Bills
Illegal Immigrants Leave US Hospitals With Billions In Unpaid Bills
By Autumn Spredemann of The Epoch Times
Tens of thousands of illegal…
Share this:

{kind=link}
{kind=link}

By Autumn Spredemann of The Epoch Times
Tens of thousands of illegal immigrants are flooding into U.S. hospitals for treatment and leaving billions in uncompensated health care costs in their wake.
{kind=link}
The House Committee on Homeland Security recently released a report illustrating that from the estimated $451 billion in annual costs stemming from the U.S. border crisis, a significant portion is going to health care for illegal immigrants.
With the majority of the illegal immigrant population lacking any kind of medical insurance, hospitals and government welfare programs such as Medicaid are feeling the weight of these unanticipated costs.
Apprehensions of illegal immigrants at the U.S. border have jumped 48 percent since the record in fiscal year 2021 and nearly tripled since fiscal year 2019, according to Customs and Border Protection data.
Last year broke a new record high for illegal border crossings, surpassing more than 3.2 million apprehensions.
And with that sea of humanity comes the need for health care and, in most cases, the inability to pay for it.
In January, CEO of Denver Health Donna Lynne told reporters that 8,000 illegal immigrants made roughly 20,000 visits to the city’s health system in 2023.
The total bill for uncompensated care costs last year to the system totaled $140 million, said Dane Roper, public information officer for Denver Health. More than $10 million of it was attributed to “care for new immigrants,” he told The Epoch Times.
Though the amount of debt assigned to illegal immigrants is a fraction of the total, uncompensated care costs in the Denver Health system have risen dramatically over the past few years.
The total uncompensated costs in 2020 came to $60 million, Mr. Roper said. In 2022, the number doubled, hitting $120 million.
He also said their city hospitals are treating issues such as “respiratory illnesses, GI [gastro-intenstinal] illnesses, dental disease, and some common chronic illnesses such as asthma and diabetes.”
“The perspective we’ve been trying to emphasize all along is that providing healthcare services for an influx of new immigrants who are unable to pay for their care is adding additional strain to an already significant uncompensated care burden,” Mr. Roper said.
He added this is why a local, state, and federal response to the needs of the new illegal immigrant population is “so important.”
Colorado is far from the only state struggling with a trail of unpaid hospital bills.

Dr. Robert Trenschel, CEO of the Yuma Regional Medical Center situated on the Arizona–Mexico border, said on average, illegal immigrants cost up to three times more in human resources to resolve their cases and provide a safe discharge.
“Some [illegal] migrants come with minor ailments, but many of them come in with significant disease,” Dr. Trenschel said during a congressional hearing last year.
“We’ve had migrant patients on dialysis, cardiac catheterization, and in need of heart surgery. Many are very sick.”
He said many illegal immigrants who enter the country and need medical assistance end up staying in the ICU ward for 60 days or more.
A large portion of the patients are pregnant women who’ve had little to no prenatal treatment. This has resulted in an increase in babies being born that require neonatal care for 30 days or longer.
Dr. Trenschel told The Epoch Times last year that illegal immigrants were overrunning healthcare services in his town, leaving the hospital with $26 million in unpaid medical bills in just 12 months.
ER Duty to Care
The Emergency Medical Treatment and Labor Act of 1986 requires that public hospitals participating in Medicare “must medically screen all persons seeking emergency care … regardless of payment method or insurance status.”
The numbers are difficult to gauge as the policy position of the Centers for Medicare & Medicaid Services (CMS) is that it “will not require hospital staff to ask patients directly about their citizenship or immigration status.”
In southern California, again close to the border with Mexico, some hospitals are struggling with an influx of illegal immigrants.
American patients are enduring longer wait times for doctor appointments due to a nursing shortage in the state, two health care professionals told The Epoch Times in January.
A health care worker at a hospital in Southern California, who asked not to be named for fear of losing her job, told The Epoch Times that “the entire health care system is just being bombarded” by a steady stream of illegal immigrants.
“Our healthcare system is so overwhelmed, and then add on top of that tuberculosis, COVID-19, and other diseases from all over the world,” she said.

A newly-enacted law in California provides free healthcare for all illegal immigrants residing in the state. The law could cost taxpayers between $3 billion and $6 billion per year, according to recent estimates by state and federal lawmakers.
In New York, where the illegal immigration crisis has manifested most notably beyond the southern border, city and state officials have long been accommodating of illegal immigrants’ healthcare costs.
Since June 2014, when then-mayor Bill de Blasio set up The Task Force on Immigrant Health Care Access, New York City has worked to expand avenues for illegal immigrants to get free health care.
“New York City has a moral duty to ensure that all its residents have meaningful access to needed health care, regardless of their immigration status or ability to pay,” Mr. de Blasio stated in a 2015 report.
The report notes that in 2013, nearly 64 percent of illegal immigrants were uninsured. Since then, tens of thousands of illegal immigrants have settled in the city.
“The uninsured rate for undocumented immigrants is more than three times that of other noncitizens in New York City (20 percent) and more than six times greater than the uninsured rate for the rest of the city (10 percent),” the report states.
The report states that because healthcare providers don’t ask patients about documentation status, the task force lacks “data specific to undocumented patients.”
Some health care providers say a big part of the issue is that without a clear path to insurance or payment for non-emergency services, illegal immigrants are going to the hospital due to a lack of options.
“It’s insane, and it has been for years at this point,” Dana, a Texas emergency room nurse who asked to have her full name omitted, told The Epoch Times.
Working for a major hospital system in the greater Houston area, Dana has seen “a zillion” migrants pass through under her watch with “no end in sight.” She said many who are illegal immigrants arrive with treatable illnesses that require simple antibiotics. “Not a lot of GPs [general practitioners] will see you if you can’t pay and don’t have insurance.”
She said the “undocumented crowd” tends to arrive with a lot of the same conditions. Many find their way to Houston not long after crossing the southern border. Some of the common health issues Dana encounters include dehydration, unhealed fractures, respiratory illnesses, stomach ailments, and pregnancy-related concerns.
“This isn’t a new problem, it’s just worse now,” Dana said.

Medicaid Factor
One of the main government healthcare resources illegal immigrants use is Medicaid.
All those who don’t qualify for regular Medicaid are eligible for Emergency Medicaid, regardless of immigration status. By doing this, the program helps pay for the cost of uncompensated care bills at qualifying hospitals.
However, some loopholes allow access to the regular Medicaid benefits. “Qualified noncitizens” who haven’t been granted legal status within five years still qualify if they’re listed as a refugee, an asylum seeker, or a Cuban or Haitian national.
Yet the lion’s share of Medicaid usage by illegal immigrants still comes through state-level benefits and emergency medical treatment.
A Congressional report highlighted data from the CMS, which showed total Medicaid costs for “emergency services for undocumented aliens” in fiscal year 2021 surpassed $7 billion, and totaled more than $5 billion in fiscal 2022.
Both years represent a significant spike from the $3 billion in fiscal 2020.
An employee working with Medicaid who asked to be referred to only as Jennifer out of concern for her job, told The Epoch Times that at a state level, it’s easy for an illegal immigrant to access the program benefits.
Jennifer said that when exceptions are sent from states to CMS for approval, “denial is actually super rare. It’s usually always approved.”
She also said it comes as no surprise that many of the states with the highest amount of Medicaid spending are sanctuary states, which tend to have policies and laws that shield illegal immigrants from federal immigration authorities.
Moreover, Jennifer said there are ways for states to get around CMS guidelines. “It’s not easy, but it can and has been done.”
The first generation of illegal immigrants who arrive to the United States tend to be healthy enough to pass any pre-screenings, but Jennifer has observed that the subsequent generations tend to be sicker and require more access to care. If a family is illegally present, they tend to use Emergency Medicaid or nothing at all.
The Epoch Times asked Medicaid Services to provide the most recent data for the total uncompensated care that hospitals have reported. The agency didn’t respond.
Continue reading over at The Epoch Times


The War Between Knowledge And Stupidity


Sylvester researchers, collaborators call for greater investment in bereavement care


“I Can’t Even Save”: Americans Are Getting Absolutely Crushed Under Enormous Debt Load


Problems After COVID-19 Vaccination More Prevalent Among Naturally Immune: Study


Illegal Immigrants Leave US Hospitals With Billions In Unpaid Bills


Looking Back At COVID’s Authoritarian Regimes


Moderna turns the spotlight on long Covid with new initiatives


Copper Soars, Iron Ore Tumbles As Goldman Says “Copper’s Time Is Now”


‘Excess Mortality Skyrocketed’: Tucker Carlson and Dr. Pierre Kory Unpack ‘Criminal’ COVID Response


Delta Air Lines adds a new route travelers have been asking for
-

 Uncategorized3 weeks ago
Uncategorized3 weeks agoAll Of The Elements Are In Place For An Economic Crisis Of Staggering Proportions
-

 International1 week ago
International1 week agoEyePoint poaches medical chief from Apellis; Sandoz CFO, longtime BioNTech exec to retire
-

 Uncategorized4 weeks ago
Uncategorized4 weeks agoCalifornia Counties Could Be Forced To Pay $300 Million To Cover COVID-Era Program
-

 Uncategorized3 weeks ago
Uncategorized3 weeks agoApparel Retailer Express Moving Toward Bankruptcy
-

 Uncategorized4 weeks ago
Uncategorized4 weeks agoIndustrial Production Decreased 0.1% in January
-

 International1 week ago
International1 week agoWalmart launches clever answer to Target’s new membership program
-

 Spread & Containment3 days ago
Spread & Containment3 days agoIFM’s Hat Trick and Reflections On Option-To-Buy M&A
-

 Uncategorized4 weeks ago
Uncategorized4 weeks agoRFK Jr: The Wuhan Cover-Up & The Rise Of The Biowarfare-Industrial Complex