The Endpoints 11: The top private biotechs in pursuit of new drugs. Pushing the envelope with powerful new technologies
Right around the beginning of the year, we got a close-up look at what happens after a boom ripples through biotech. The crash of life sciences stocks…
Right around the beginning of the year, we got a close-up look at what happens after a boom ripples through biotech. The crash of life sciences stocks in Q1 was heard around the world.
In the months since, we’ve seen the natural Darwinian down cycle take effect. Reverse mergers made a comeback, with more burned out shells to go public at a time IPOs and road shows are out of favor. And no doubt some of the more recent arrivals on the investing side of the business are finding greener pastures.
The fast money crowd will find something else to do, for a time. And what one biotech investor once described to me as the “comic book” biotechs will be gone.
The best of the private startups, though, have continued to thrive in a more difficult fundraising environment. The most important factors in new drug development — more powerful computational power matched with fresh insights into what triggers disease — are opening doors that we never exactly knew existed even a few years ago.
The first experts through those doors, and on to new drugs, stand to benefit enormously. And that’s a big motivation for continuing biotech investment.
One of the regular themes you’ll see in this year’s list of the most notable private biotechs in the business is the willingness to leap into next-gen therapies — an eagerness to take some mighty risks in order to find new drugs that are better for patients and easier to make. Open one door in this business and you’ll find more on the other side, begging someone to try the knob.
It’s never been more obvious just how essential biotechs are to new drug development. As Big Pharma is more fixed than ever on de-risking and late-stage drugs, true discovery work will be left to the upstarts to break new ground. Even in the area of trial design, where Big Pharma would seemingly have the most to gain immediately, it’s the smaller companies that are exploring game-changing new strategies, as you’ll see below.
This year’s group of the Endpoints 11 has a wide mix of players. Altogether they represent the best of biotech — and a good example of why biotech’s current disfavor on Wall Street is just another temporary trend.
The Endpoints 11
Affini-T Therapeutics: “A straight path to a drug approval”
Altos Labs: This startup is breaking all the rules
Areteia Therapeutics: ‘God is in the details’
Generate Biomedicines: “You’re talking 20 to the 200th power”
Mammoth Biosciences: “Suddenly the world is your oyster”
Metagenomi: ‘I’m very interested in the search for the unknown’
Neumora: Going big, or going home
Odyssey Therapeutics: ‘Here it’s enhanced and scaled’
Orna Therapeutics: The O is circular
Rome Therapeutics: A voyage into the dark genome
Versanis Bio: Some things never change
1. Affini-T Therapeutics: “A straight path to a drug approval”
Jak Knowles is tapping a network he’s been building from his early days in biotech.
↑
CEO: Jak Knowles
CSO: Loïc Vincent
CMO: Dirk Nagorsen
Based: Boston/Seattle
Backers: Vida Ventures and Leaps by Bayer led its $175 million round in March, with support from the Humboldt Fund, The Parker Institute for Cancer Immunotherapy, Catalio Capital Management, Agent Capital, Alexandria Venture Investments, Erasca Ventures, Fred Hutchinson Cancer Research Center and others.
The scoop: Jak Knowles’ original life plan focused on a career as a surgeon. But during a research stint at Memorial Sloan Kettering he had a chance to do work at ImClone, while it was developing cetuximab. By the time his residency had started, he was prescribing it.
“It really showed me how fast you can have something translate from the bench side, from the lab to the patient care,” Knowles says. “So that really got me excited and it gave me, I think, a little extra motivation when I was feeling like my surgical training was not satisfactory … to leave and pursue a career in biotech.”
Todd Foley
And he decided to tackle it from the ground up, where he had the chance to work with some game-changers in the field early on.
His first foray into the biotech world came at MPM Capital, where “Todd Foley taught me everything I know about term sheets and contract negotiation.” Then he moved to CureDuchenne. His first investment was in Bamboo Therapeutics, a spinout from Jude Samulski’s AskBio. Pfizer bought it seven months later in what Knowles described as “the fastest exit of my life.”
Phil Greenberg
Then came an interim CEO role helping create another wunderkind biotech — Exonics, later bought out by Vertex — and then he jumped to the helm of a natural killer cell company called CytoSen, which sold to Kiadis and ended up at Sanofi.
But he was just getting started making connections. He jumped to Leaps by Bayer, working with Jürgen Eckhardt, which put him on the inside of a brash gene editing player called Metagenomi, where he did a stint as chief business officer.
Which brings us to today, where Knowles is co-founder and CEO at Affini-T, a Fred Hutch spinout pinning its hopes of ultimately tackling solid tumors by using Affini-T’s T-cell receptors with a CD8 co-receptor to build enhanced CD8 and CD4 T cells that promise to work longer and harder than the first-gen cell therapies now out on the market. Together, the approach has shown promise in the lab to drum up some cytokine support and get dendritic cells to recruit more T cells to the fight. The biotech was founded by 3 key scientists — Juno co-founder Phil Greenberg, Aude Chapuis and Tom Schmitt — looking to create a cell therapy 2.0 player.
Aude Chapuis
They’re tackling a key oncogenic driver, KRAS, where the biotech believes there’s much, much more therapeutic potential than the limited range we’ve seen with Amgen’s Lumakras G12C niche approach, using T-cell receptors to home in on their target.
And Knowles’ circle of friends and associates plays a big role in how he’s building the company. Leaps by Bayer is an investor, and they’re also collaborating with Metagenomi, which is coming up with some bespoke tools for the kind of ex vivo work Affini-T is doing to drive their next-gen therapies.
Another backer, Arjun Goyal at Vida Ventures, sees it as a crucial alliance that can allow Affini-T to pursue both autologous (extracted from the patient) and allogeneic (off-the-shelf) TCR programs for KRAS G12V and KRAS G12D, as well as other KRAS and oncogenic drivers.
Knowles believes they’ve carved out a unique strategy.
Tom Schmitt
“For our lead program against KRAS G12V, there are no medicines really even in preclinical development,” he says. “It’s very hard to develop a small molecule to that mutation. And so a TCR approach might be the only way to target KRAS G12V.
“Rarely have I seen an opportunity where there’s such a straight path to a drug approval. KRAS is a fantastic target. All of us in the oncology space have been thinking about ways to drug this target for decades.”
After getting advice for years from more senior execs, Knowles now has some thoughts of his own on building a biotech — and the kind of network that can sustain it.
“It’s a small sandbox,” he offers. “We all have to play nicely together, but I think the strong academic foundation is really the lifeblood of what we do in biotech and been very privileged, grateful to work with excellent scientists like Phil.”
For the present, at least, building a biotech likely remains sitting on the sidelines of the public market.
“Where we are right now: We came off a sugar high, very cheap capital for over two years. I think those of us who are been investors for awhile recognize that was not sustainable,” Knowles says. “And I think where we are now, it is definitely a little bit of a hangover from that party. But I don’t expect it to last.”
2. Altos Labs: This startup is breaking all the rules
“It’s about resetting the cell to this state of optimal cellular resilience.”
↑
CEO: Hal Barron
Chief scientist: Rick Klausner
Based: San Francisco,San Diego, Cambridge, UK
Backers: Altos is being a bit coy about its $3 billion commitment. Jeff Bezos is reportedly involved and Bob Nelsen at ARCH is on the board. Money, though, is not a big concern.
Rick Klausner
The scoop: Hal Barron and Rick Klausner are old friends. They’ve sat on the same board, done deals together, and share a common fascination for the big goal — the breakthrough moment, or eureka factor, whatever you want to call it, that points to new ways to treat disease.
And this time they are closely allied on the mother of all holy grail quests.
Once we heard that Altos Labs has a $3 billion commitment from backers — reportedly including Jeff Bezos — and a goal of resetting the clock on your cells, the scoffing began almost immediately on BioTwitter.
But this is too important to just shrug off as some billionaire’s loony quest to have it all, forever.
Frances Arnold
If they are even half right about what they’re capable of, the consequences in terms of disease and healthy life spans would be radical.
So let’s give Klausner and Barron — the former head of the NCI and Gates, allied with the former head of R&D at GSK — a break. The Endpoints 11 is all about swinging for the fences, and this time it’s the fences, the parking lot and the freeway beyond.
Hans Bishop, of Juno fame, is president, co-charman and founder.
David Baltimore
And they have three Nobel Prize winners on the board: Frances Arnold, David Baltimore and Jennifer Doudna. A fourth Nobel winner, Shinya Yamanaka, is senior science advisor.
Plus there’s board member Bob Nelsen, the ARCH chief who enjoys nothing more than radical R&D ambition and anything related to healthy — and potentially longer — lifespans.
Typically, for anyone running a newborn biotech, the bulk of your time is devoted to raising more money, forming alliances, gaining credibility for your work. In this case, the money is ready, and the big challenge has been creating what is essentially a new research institute spread around the globe, working on a breakthrough involving cell rejuvenation.
As for the biotech-building side of the business, they’re breaking the industry mold.
Jennifer Doudna
Toggling around the internet about Altos and its key players, you tend to pick up a lot about Yamanaka factors and the work of Juan Carlos Izpisua Belmonte in pushing back the age of a cell. That’s just part of the story, though, Barron and Klausner told me in a joint interview.
Keep in mind, both Barron and Klausner have been thinking long and hard about creating cell resilience, long before they came to Altos.
Here’s Barron:
“When you think about most companies and you talk about how they have to rush to the clinic, how they have to raise money, one of the things that differentiates us that excites me a lot is the fact that when you think about typical drug discovery and development, you try to understand the pathophysiology of a disease and you try to develop reagents, medicines, hopefully someday that actually modify that pathway and sort of slow down the progression, if you will. And that’s if it works, terrific success, and that’s the model and it makes a lot of sense.
Shinya Yamanaka
“Another way of thinking about disease, which is really unique — I think we haven’t really even contemplated this in science and medicine — is to think about the fact that when we’re young or before our bodies experienced an overwhelming amount of stress, that we’re fine. Our cells in our body and each of our organs are able to maintain what we call homeostasis. They’re able to respond to stress and stay fit, stay healthy. Whether you call this buffer capacity or resilience or cell health, there’s this concept that the cells can withstand these stressors.
“As the stressors mount, which could be everything from insulin resistance over time, it could be hyperlipidemia over time, it could be genetic stressors, autosomal recessive diseases and dominant diseases that manifest themselves over time, or even just time itself, the cells become less able to maintain homeostasis, less resilient, if you will, and they lose their healthy state.
“The concept behind Altos that I’m super-excited about for lots of reasons is that if we understand what’s enabling cells to remain healthy, this buffer, if you will, this resilience, and we’re able to actually focus on that, that’s somewhat disease independent. It’s beyond the pathophysiology of that disease. It’s rejuvenating the cells’ one way of obtaining that, but it’s basically creating a state where the cell is able to withstand the stressors that it’s experiencing. If you think about what that could do, clinically, this could actually be reversing disease, getting you to a state back when your cells were able to with stand the stresses of life.”
Here’s where Klausner steps in after I queried him about the Yamanaka factors:
“The Yamanaka factors, per sé, whether we’re ever going to use them, we use them in the lab, we don’t know. You said this has been going on for 20 years with Yamanaka, but actually that’s not true. Remember what happens with what Shinya discovered is that any cell of any age can be reprogrammed to lose their entire identity and to actually have their quote “age” reset to zero, what is probably zero post fertilization. Almost everything Shinya and everyone else has done in that field is to focus on the dedifferentiation and then the ability to create regenerative medicine from making new differentiated cells from these iPSCs. As Shinya told me before I called him about this, he said he never thought about the rejuvenation part of it and now he says, he can only think about that.
“What we’re actually beginning to see is that Yamanaka process is like a two-step process where you first rejuvenate, reset the functional fidelity of cells, reset as we’re seeing their resilience, which is how you reset a whole collection of interacting stress pathways. So it’s a very complicated biologic state. Then the Yamanaka factors, if they’re still there at some low frequency, you then go past rejuvenation of differentiated cells to the iPSC. We’re not interested in that second part. In fact, what we’re looking to do is to finally understand the molecular basis of that first step and what we’re already seeing, I’ll tell you, is that you can get totally beyond the Yamanaka factors by beginning to understand that biology of the ability to epigenetically reprogram cells. By the way, we now know, from actually people that are in Altos now, that this can happen spontaneously. This can be a physiologic process without Yamanaka factors that can be the result of cells signaling that put cells into quote, “an old state versus young state,” and we can actually toggle back and forth.
“It’s about resetting the cell to this state of optimal cellular resilience so that the stresses — be they genetic or acquired or injury — are read by the cell in a way that the cell is able to maintain homeostasis despite the stress. Again, going back to what Hal said, I have this slide, which is this is a new way to just think about most human diseases, maybe all. You only get diseases when a stress, be genetic or whatever, overwhelms. So you have two curves. The stress goes up and the resilience of the cell goes down. When those cross and the cell can’t maintain their normal function, that’s when you get disease. That’s why there’s this time dependence of disease, including of inherited genetic diseases.
Juan Carlos Izpisua Belmonte
“We never thought, I never thought in 45 years of being in this business that we can do anything other than dial one of those curves, the stress curve. But Juan Carlos’ data and now lots of other people, actually showed, whoa, there’s mechanisms in the cell where you can reset not the stress curve, but the resilience curve. That’s new and that’s the basis of Altos.”
To get there, the two Altos founders are building a global institute which has already recruited more than 300 people for the organization, bringing in entire labs in the process. By the end of this year, that could swell to 400.
“The growth after that will obviously be much slower,” says Barron, “but some of it will depend on our success. Some of it will depend on which projects go which direction in terms of the types of people we’d need. But what our strategy for being global is because if you really believe in the model, which we do, the best people in the world, they’re not going to be conveniently located where your headquarters are.”
For a company with global ambitions on creating a whole new kind of biotech, the sky’s the limit.
3. Areteia Therapeutics: ‘God is in the details’
Clive Meanwell has figured out a few things about late-stage R&D
↑
CEO: Jorge Bartolome
CSO: Calman Prussin
Based: Pittsburgh
Backers: Population Health Partners and Knopp Biosciences created the company with a $350 million launch round. The syndicate is led by Bain Capital Life Sciences and loops in Access Biotechnology, GV, ARCH Venture Partners, Saturn Partners, Sanofi, Maverick Capital, and Population Health Partners.
Calman Prussin
The scoop: R&D trends over the last decade have not been kind to major market drugs. It’s precisely those therapeutics that are most likely to fetch the biggest returns that are often neglected because they are left to the Big Pharma players to work with. Biotechs typically can’t handle the load the FDA has required in terms of safety and efficacy data.
And let’s face it, the biggest players can be painfully slow, tradition-bound and often mired down by legacy tech and outlook. All in ways that add to the cost, and detract from the appetite.
One of the biotechs out to change that — along with the whole late-stage dynamic — is Areteia Therapeutics. This is one of those stories that starts with a team of people who never lost hope in the therapeutic power of a failed drug. And their partnership with some deep-pocket players has put them in play, lining up a late-stage test that many would find daunting.
Ian Read
Nobody knows that better than Ian Read, the former CEO at Pfizer, who knows firsthand what it’s like staring down a $1 billion or $2 billion bill for a clinical trial. He’s the chairman at Areteia and a partner at Population Health.
“It was culturally difficult in Big Pharma to remove costs both because they’re stranded and because you have a global reputation to protect and you have to make sure that your regulatory and your safety and everything is done par excellence, which leads to redundancies,” Read tells me. “Not saying that our approach is less secure, less focused on safety, but it’s just easier to implement, I think.”
Read’s focus now is shaped by Population Health Partners, where he works with Clive Meanwell on shaking up the old paradigm. And along with a few deep-pocket players like Adam Koppel at Bain, they’re taking a calculated risk backing Areteia’s Phase III quest on a new asthma drug.
Clive Meanwell
There are a lot of people in drug development who “want to measure everything lots of times,” Meanwell tells me in an interview with Read. “When I was doing cardiovascular trials earlier in my career, I’d often have big fights with very important cardiologists, including the one who currently runs the FDA, where you’d say, ‘Why are we measuring all this stuff so often? Do we really need to?’ And it was a very important fight to have, because you’d go from 500 independent variables per patient, to 250. That may not sound dramatic, but if it’s in 20,000 people, it starts to add up and everyone needs a blood test. And every blood test needs to be checked and every check needs to be double-checked. This is what drives a lot of the costs. I can remember knocking out $14 million of lab tests in one study by just arguing these very basic ideas. And we need to recognize that these trials have to have simple objectives and simple measures.
“Now God is in the details. It’s not really a secret sauce. It’s just ask the question, why is it so expensive? Should it be so expensive? If your complete focus is on time, you might not ask that question very seriously. And if you’re worried about quality and your notion of quality is do everything three-fold, which is not really most quality experts’ notion of quality — it’s not repetitive observation. It’s reliability of observation. Then you also have a different way. So the last thing I’ll say on this point, because I think it’s really important, is that what brings efficiency is the motivation for efficiency, which is purposefulness. If you are doing a trial that’s important, then it’s easier to do it efficiently.”
It’s still not cheap to do a billion-dollar trial for a third of that cost, but it is more in the range of the deep-pocket investors behind Areteia. And they’re taking that strategy and using it to develop a drug called dexpramipexole, which Biogen left for dead after a failure in treating ALS.
Mike Bozik
That setback left the drug in the hands of Knopp Biosciences CEO Mike Bozik, who persevered in believing that a clear signal on an eosinophil effect could be translated into a pivotal win that would set the stage for a significant market launch in asthma — where a very effective pill could make hay in a field dominated by biologics.
Bozik pushed that belief all the way through a proof-of-concept clinical study, and then the backers came in for the big test. And for Meanwell, that also includes doing a much better job at recruiting precisely the people you want, where they are being treated in general practice.
All of the people here, whether it’s on the Knopp team that kept the faith, Meanwell and the investors he’s won over after a great run at The Medicines Company, the team they recruited to make it all happen, share in creating an interesting gamble — one that could ultimately be far more influential than any single disease gambit.
And that’s worth paying very close attention to what happens next.
4. Generate Biomedicines: “You’re talking 20 to the 200th power”
Generate is promising to bring new technology to bear in a radical improvement of discovery efficiency
↑
CEO: Michael Nally
CMO: Alexandra Snyder
Based: Somerville, MA
Backers: Flagship Pioneering founded the company and raised a $370 million round last fall with the Abu Dhabi Investment Authority, the Alaska Permanent Fund, Altitude Life Science Ventures, ARCH Venture Partners, Fidelity Management & Research Company, Morningside Ventures and funds counseled by T. Rowe Price Associates.
The scoop: We’ve heard plenty of boasting from the AI and machine learning crowd about their ability to find new drugs in record time. Now we’re getting to the point where the rubber hits the road on human data, and Generate Biomedicines promises to bring the full weight of the Moderna-enriched group at Flagship Pioneering to bear on that front.
Geoffrey von Maltzahn
Like most of Flagship’s investments, this biotech was born in the Flagship labs several years before the coming-out party. A trusted Flagship insider, Geoffrey von Maltzahn, is a co-founder. Flagship chief Noubar Afeyan chose this as one of the portfolio companies where he’s serving as chairman. And — in what is now classic Flagship style ‚ brought in a longtime industry vet to lead the way.
“So we were 30 when I started 18 months ago,” CEO Mike Nally tells me. “We ended the year around 90 (staffers). Today we’re at 215, going to end up probably 260 to 270 by the end of the year, and on track to continue to scale as we go into next year. If you think about the kind of components, the computational piece was first, building that foundation. That has now scaled. The protein sciences group has been built up. Now we’re working on the preclinical sciences group. And then ultimately we’ll move into the clinical development and CMC spaces.”
Noubar Afeyan
Like the rest of the AI/ML crew, Generate is promising to bring new technology to bear in a radical improvement of discovery efficiency, relying on its study of a vast swath of proteins to help point to new medicines.
“If you think about the convergence of computing power, machine learning techniques, but also the underlying data set that we trained our models on, the protein data bank has matured massively,” Nally adds. “That gave us 200,000 high resolution protein structures. The genomics revolution gave us the amino acid sequence, 190 million of them across all the trees of life. The computing power a decade ago, it would’ve taken a hundred years to train our core model, with the cutting-edge, state-of-the-art computers. Now we can run that almost instantaneously. And so it’s truly this convergence of computing power, it’s this convergence of machine learning techniques, but also high-quality data to actually analyze.”
Their initial focus switched to Covid-19 as the pandemic reoriented R&D to the greatest immediate need, with an immunology program “not far behind.”
Alexandra Snyder
“We actually went out and targeted the conserved regions of the spike protein, and the structural biologists split the receptor binding domain into four different regions,” Nally says. “The class four region has been remarkably conserved, but there’s also two other regions, the NTD non-supersite, as well as the S2 domain, that have largely been conserved across viruses. And so we said, could we use the specificity of the technology and drive not only strong binding, but ultimately neutralization at those sites. The S2 antibodies that we’ve developed now seem to neutralize all existing variants of concern.”
When Nally joined Generate, the biotech was still small, hardly enough to fill a tiny group at giant Merck, where Nally had toiled for 20 years, ending as marketing chief. To hear him tell it, though, he’s relished every bit of it.
This first program doesn’t use a novel drug. Instead, they’re taking an existing antibody — tezepelumab — and amping it up for use against Covid. And that’s where some of the low-hanging fruit can be found.
“One of the beautiful things about the technology is it allows us to co-optimize molecules and drive functional improvements of five, ten-fold quite regularly,” Nally says. “And so our ability to search protein spaces is one of the really fascinating things. If you think about traditional approaches, when you think about where the IP landscape resides, it’s in the CDR region (complementarity-determining regions) of an antibody. Traditional techniques, if you make one or two changes to the CDR, usually you lose function.
“What our technology allows us to do is actually change up to 70% of the CDR, while retaining our enhancing function. And that’s just a way of exploring this vast protein space, which when you think about what nature has sampled in terms of proteins, Frances Arnold (a board member) said this to me when I was looking at Generate. She said, “Mike, for all of its majesty, nature has sampled one drop of water in all the ocean of potential proteins.
“The average protein being 200 amino acids long, 20 different choices at each amino acid’s spot, you’re talking 20 to the 200th power. That’s more than the atoms in the universe squared. And so our technology allows us to search that broad landscape and find functional alternatives.”
That kind of tech creates a big platform, in an arena where big platforms are the norm. It also creates some big questions about choice.
“I think there’s three different kind of phenotypes,” says Nally. “One is, can we apply machine learning, artificial intelligence, to small molecules? And you’ve seen a number of different companies in that space. We’ve also seen a number of companies go into AI/ML for target discovery. Our organization focuses on the protein modality, and what the team was able to ascertain is that there are generalizable principles that govern protein function. And by understanding those principles, it allows us to program novel proteins across all protein modalities. So antibodies, bispecifics, peptides, enzymes, cell gene therapy, all have a protein modality or protein foundation. And then when you think about it, this works across all disease areas. So a huge part of our challenge is choice.”
To hear Nally tell it, the increased complexity of drug research is reaching the outer limits of our individual knowledge about developing new drugs. This next generation needs the added computer power of AI/ML. And he intends for Generate to be at the forefront of that movement.
5. Mammoth Biosciences: “Suddenly the world is your oyster”
Backed by Jennifer Doudna in a world still waking up to gene editing’s potential, Mammoth has some big ambitions
↑
CEO: Trevor Martin
CSO: Lucas Harrington
Based: Brisbane, CA
Backers: The $150 million D round last fall was led by Redmile Group, with participation from Foresite Capital, Senator Investment Group, Sixth Street, Greenspring Associates, Mayfield, Decheng Capital, NFX and Plum Alley.
The scoop: Nobody knows better than the crew at Mammoth Biosciences how important CRISPR/Cas9 has been to birthing the gene editing field. And no one knows better than the folks running this Jennifer Doudna startup just how much the field still needs to be developed.
Lucas Harrington
Talking with Trevor Martin, brimming with youthful enthusiasm, the next-gen approach seems inevitable.
“Our philosophy at Mammoth is that it’s really about having the broadest toolbox,” says the Mammoth CEO. “So that’s the foundation of the company and as we’re building and pioneering these next-generation therapeutics and diagnostics, everything ties back to this toolbox … where you can have the hammer and the screwdriver and the wrench and the ruler.”
Too many times, he says, a biotech takes one tool and builds the company around it — even as the technology around building tools changes.
“Maybe they license on a university or whatever it is and everything has to revolve around that,” he says. “I think we take a very broad view, and that started at the beginning of the company, where we pioneered this whole new field of CRISPR-based diagnostics and we just take this really broad view of CRISPR generally — where it’s not just a gene-editing tool.
“We have this concept of Mammoth of what we call CRISPR-plus and that’s how do we combine the CRISPR systems with other functionalities, whether that’s things like base editing or that’s activating or inhibiting. And once you start thinking about CRISPR as this kind of search engine for biology and this way of programmatically sending proteins anywhere you want to any DNA and RNA, like suddenly the world is your oyster — whether it’s diagnostics or therapeutics or subclass of therapeutics. And I think that’s built into the DNA and RNA of Mammoth and that’s one of the things that really makes us unique.”
The toolbox now includes miniaturized Cas14 as well as CasΦ, which is used to overcome some of those Cas9 limitations with greater versatility.
Janice Chen
It’s a young crowd, at least by your average gray-haired norm seen in most biotech C-suites these days. Stanford-grad Martin was 29 when he co-founded the company about five years ago with Janice Chen and Lucas Harrington.
But with Doudna heading up the scientific advisory board and the world still waking up to the fast-changing world of gene editing, the company gained early credibility. It didn’t hurt that Tim Cook at Apple was an initial investor. And 10 months ago, Vertex, with its deeply respected research team and game-changing aspirations to create new cures, signed on with a partnership that totaled $700 million in size. Bayer also signed up for a collaboration, and while Martin still isn’t saying much about what they’re working on, he’s all in on what they are trying to do here.
Mammoth, he says, is “really focused especially on in vivo (in the body) and this idea of permanent genetic cures, like one-time treatments.”
Curiously, Mammoth already has an approval to its credit, with a Covid diagnostic greenlit in an emergency use authorization from the FDA. But it’s still not quite ready for prime time, as Mammoth works on a more decentralized test for broader use.
“This is something that was just in the lab a few years ago to go all the way through and going head-to-head with the established technologies like PCR,” says Martin. “And one of the really cool things is that the FDA’s emergency use authorization sheet then added CRISPR as a category, right next to these technologies that have been around for decades and decades. And I think that’s a testament to the power of the technology and also the immense work of the team, night and day, to get that done, and I think it’s a huge milestone in terms of really benchmarking where CRISPR diagnostics fits in the overall diagnostic landscape.”
6. Metagenomi: ‘I’m very interested in the search for the unknown’
A seminal collaboration at Berkeley laid the foundations for this biotech
↑
CEO and founder: Brian Thomas
CMO: Alan Cohen
Based: Emeryville, CA
Backers: PFM Health Sciences, Farallon Capital Management, and a “leading global investment firm” led the last round. New investors included Eventide Asset Management, Deep Track Capital, Frazier Life Sciences, Pura Vida Investments, Irving Investors, Millennium Management, Surveyor Capital, Marshall Wace, Novo Holdings A/S, and Bristol Myers Squibb. The raise also included money from Moderna, a partner, as well as the early investors: RA Capital Management, Leaps by Bayer, and Humboldt Fund, among others.
The scoop: To understand what motivates Brian Thomas, the CEO at Metagenomi, you have to go back to the mid-90s, when he moved from his native Kansas to do his postdoc at Berkeley.
Alan Cohen
“I walked around Berkeley for three weeks with my eyes wide open, and fell in love with the area and said I was never going to leave. I did my postdoc here with a guy named Norm Pace. (Pace was profiled by Ed Yong at The Atlantic a few years ago, credited with revolutionizing the study of life.) And that’s where I really got interested in the search for the unknown; this search for this life on this planet that we don’t know about. And that to me, really kind of stimulated a lot of my early formative scientific years.”
Next-gen sequencing led to a completely new understanding of the genome, helping spawn bioinformatics and the kind of massive computer power needed to drive that work. And then his exploration of the unknown led to Jill Banfield, credited with opening up the scientific doors that led Jennifer Doudna to her discovery of CRISPR/Cas9 with Emmanuelle Charpentier. Today, Doudna and Banfield still collaborate, now partnered on a startup called IGI, which is using gene-editing tech to alter the microbiome to help control the level of carbon animals create, and plants devour.
Norm Pace
After a stint in industry, Thomas would return to Berkeley. “And the last 12 of those years was exclusively working with Jill,” he says, “just because of the real amazing technology of metagenomics and what it can tell you.”
For Thomas, it would be another eye-opening experience, which ultimately led him to start a company that would explore nature in search of a multitude of nucleases to create bespoke tools for gene editing — in vivo and ex vivo.
Initially, the work at Berkeley involved studying what he calls “limited” or “restricted” environments. But as the tech advanced, they could delve into more complex areas.
Jill Banfield
“Then the partnership with Jill became really important, because we started to hit these regions in the genome of these organisms that we’ve never studied before, that were highly repetitive. And so we started to see that motif of this repeat/something, repeat/something, repeat. We actually had a couple of papers where we looked at: What is in the sequence between those repeats? And what is it all about? And that’s what started to give us this idea, that these viral defense mechanisms are.” He pauses for a moment and regroups.
“They actually have a time snapshot, which was fascinating, so there’s an end to them. So, if you think about it, you’ve got a repeat and then this spacer region, and it goes on for some number of repetitive elements, but the spacers are different in between. And when you look at those spacers, the thing that gave us a clue as to what these were doing, and this was before CRISPR was a household word … We started to get hits in those little regions of this bacterial genome to a virus genome. And we started to think: Why are there chunks of virus genome inserted into the bacterial genome? And that’s what led us kind of further. I think that’s essentially the beginnings of the relationship that Jennifer Doudna and Jill built with our two groups.
“And then, I think it was the paper that we had back in, I can’t remember now, 2016, 2017, that showed that we could use metogenomic data to source novel gene editing systems. And so, we were able to show that quite well. And I think then, that kind of leads you … right to Metagenomi.
“I think the database that we’ve built, from probably one of the biggest, if not the biggest, metagenomic database that’s out there. It’s filled with solutions. And so, what we can do quickly? Metagenomi can find those solutions, and we can rapidly develop those into technologies that are going to be important.”
For Thomas, it was all part of a journey that would persuade him to leave his beloved academia. He felt going into a startup offered a chance to drive the technology more quickly. A $175 million round at the beginning of this year — bringing the total raise to $300 million — along with a pact with Moderna that’s drawn plenty of added attention, has validated that decision.
“I’m very interested in the search for the unknown,” says the CEO. “Being able to tap into these life forms that we’ve never really known about. I think to me, it’s a very relatable story. You’ve got a backyard, you’ve got soil in that backyard. You go out into that soil, and there’s unknown life there. We think we’re really smart about biology. We think we know a lot about microbes in the environment and everything, but we don’t. I think that’s the part that kind of drew me this way. And it’s been a passion of mine from the very beginning.”
7. Neumora: Going big, or going home
Absorbing biotechs, programs — and people — from Amgen, ARCH has big plans for the RBNC
↑
CEO: Paul Berns
Head of R&D: John Dunlop
Based: Watertown, MA/Brisbane, CA
Backers: Neumora made its public bow with $500 million credited to its accounts, the kind of splashy intro ARCH loves to make with its startups. The VC provided much of that themselves, with a $100 million equity stake coming from Amgen. The other players: Alexandria Venture Investments, Altitude Life Science Ventures, Catalio Capital Management, F-Prime Capital, Invus, Logos Capital, Mubadala Capital, Newpath Partners, Polaris Partners, re.Mind Capital (Apeiron), Softbank Vision Fund 2, Surveyor Capital (a Citadel company), Waycross Ventures (Byers Capital) and “other undisclosed investors.”
The scoop: The folks at ARCH don’t much care to mess with anything small. But when they go big, there’s nothing wild about it. They like to think through the odds, calculate a reasonable path to proving something in the clinic. And by the time Neumora was polished up and ready to roll out of stealth, you could see that the strategy was fully fleshed, with drugs already in the clinic.
John Dunlop
Rather than bake everything in the pipeline from scratch, Neumora came in with drugs from other companies to prime the clinical pump.
“Our lead program is kappa-opioid receptor antagonists,” says Carol Suh, a co-founder and SVP of strategy at Neumora. “It’s in Phase II clinical trials targeted for depression. We’re really excited about that one actually. J&J also has a program that they’ve showed a positive signal in their Phase II. And it further validates the target clinically. So we’re excited about being able to progress that forward and really bring in a novel class of targets for depression.”
There are other areas Neumora is exploring that are shared by other developers. The biotech recently allied itself with a team at Vanderbilt, in-licensing an M4, where Karuna recently enjoyed a spectacularly, and singularly surprising, success with an M1/M4 drug. Cerevel and Neurocrine are also active in this arena.
Carol Suh
At this biotech, not having the most advanced type of drug in development doesn’t mean that it can’t end up with the best, or find a particular patient niche which would benefit more than other categories.
“So let’s say for our clinical stage programs that are already in flight that we’ve in-licensed, there are opportunities for us to further determine (patients) through our data science approaches,” Suh says. “Are there really interesting enrichment strategies? Are there different subpopulations we can better target? How do we think about defining our clinical trial design in that way?
“But aside from the data science approaches, we still think fundamentally what’s important is, having really good, solid assets, solid molecules that we know have really strong biological rationale and even clinical validation. That because these markets are so big and that there’s so many patients in need, that there’s opportunities for a number of different players. And we believe to be able to show best-in-class potential.
“We believe it’s like an all-ships-rise type of scenario, that there are still also multiple opportunities for multiple programs in this space as well. And these are really just treatments seeking patient populations as well. So again, we’re just really excited about the advancements that we’ve seen with Karuna and with Cerevel as well. And we think that there’s an opportunity for us too.”
Suh and her colleagues subscribe to the notion that neuroscience has made real advances in the past five years, with advances opening doors that weren’t visible until recently. After the debacle with Aduhelm, it’s easy to believe that the whole field around neurodegeneration is nothing but a disaster zone, luring in one big attempt after another to beat Alzheimer’s with the (frequently discredited) amyloid beta theory. Neumora’s interest in psychiatric drugs — dominated by therapies that are often hit-and-miss — could also be seen as a long shot.
But when you talk to them about that, you get the idea that you haven’t been paying close enough attention to the science. Like in depression and anxiety, a field where millions of desperate patients are either not being treated or treated inadequately.
“We have a vasopressin 1A receptor antagonist that’s currently in Phase I trials. We’re looking to pursue that program in the field of anxiety disorders,” Suh says. “We believe that there’s an anxiolytic effect and we’re continuing to progress the program.”
In some respects, Neumora represents the cutting-edge in drug science that the industry depends on. Big Pharmas either get stuck on the wrong working theory or abandon it entirely. Like Pfizer and Amgen. But both Pfizer and Amgen also recognize that Big Pharma pipelines are a poor home for many of these experimental drugs — and they’ve both out-licensed programs to smaller, more focused biotechs like Neumora. Amgen did that with Neumora, and the biotech also works together in collaboration where that makes sense.
ARCH is backing this one to the hilt, gathering a half billion dollars to walk the walk in clinical development. Everything isn’t going to work here, or won’t happen before rivals come out with something better. But in a field ripe with this many targets of opportunity, they don’t have to be right every time.
8. Odyssey Therapeutics: ‘Here it’s enhanced and scaled’
This time Gary Glick is scaling up the pipeline, and he means to go big and long
↑
CEO: Gary Glick
EVP, cancer biology: Robert Abraham
Based: Boston, MA, Ann Arbor and Frankfurt
Backers: The $218 million launch round was led by OrbiMed Advisors and co-led by SR One Capital Management with help from Foresite Capital, Woodline Partners LP, Logos Capital, HBM Healthcare Investments, Colt Ventures, Creacion Ventures, “and other institutional investors.”
The scoop: If there’s anyone in biotech who knows a thing or two about building a biotech, working on new drugs and then forging an M&A or licensing deal around it, it’s Gary Glick.
Robert Abraham
Glick has built and sold a string of drugs. He did it with Lycera. He did it with IFM, twice. He launched Scorpion with the help of his old compadres at Atlas, and then he went off to launch Odyssey.
This time, as the name implies, he’s in it for the long haul. And he has some deep-pocket investors who believe he’s going to make it.
Two years after quietly hiring his first staffer, Odyssey now has a staff of 160. He credits his team with 35 approved drugs and hundreds of clinical forays. And he plans to put the engine he’s been building to work on scaling up.
“We have nine programs, pipeline programs,” Glick tells me. “The first three will be in the clinic in ’24. So the next several will be in ’25 and something in ’26. We’re working on a couple different partnerships right now with large pharma partners. We have, I think, probably about five different sort of key technology platforms that are sort of broken up into three main areas to help support that. We have target discovery, 160 people, lots going on.”
Immunology, and Glick has a ton of experience in inflammation, is in play. So is oncology.
Jeff Leiden
Their team includes Jeff Leiden, the iconic ex-CEO at Vertex, now chairman of the board at Odyssey. The ex-Pfizer cancer expert Robert Abraham — with 10 cancer approvals to his credit — arrived at the company via Vividion, which was acquired by Bayer. Novartis vet Shifeng Pan — who is credited with a leading role in three drug OKs — runs discovery. Another Novartis vet, Natalie Dales, is an EVP. The list goes on.
To accommodate them, he’s acquired facilities in Cambridge, MA, a familiar spot for Glick in Ann Arbor, MI and Frankfurt, Germany.
Shifeng Pan
“We’re probably more heavily focused today on the immunology side of the world that we want to be first, second, or perhaps third to the market with our compound,” says the CEO. “So we’re not going to be a fifth best-in-class. That’s just never going to be something we do. We want to be able to work on projects or targets that we think will lead to revolutionary, or really generational changes, exceptional changes in the standard of care. And that is, I would say, the sort of key features that differentiates Odyssey. We are working on some very hard projects. No drug discovery is easy. But on the spectrum, we are tackling some of the things that others have shied away from.”
And this time around, he’s not looking for any fast exits.
“It’s not meant to be sold,” says Glick. “It’s meant to be a sustainable organization that 10 years from now, 15 years from now, is going to be around … Everything here is homegrown like all of my other companies. I learned how to do that at Lycera. Refined it at IFM. Took it to Scorpion and here it’s enhanced and scaled.”
Natalie Dales
Glick protests that he never set out to flip companies.
“It just happened that way,” he tells me. “I mean, six months after you start the company, someone puts a $2.4 billion term sheet on the table. It’s like, ‘Okay.’
“There’s a lot of very interesting things out there, but we’re right now focusing on small molecules and proteins, since they’re more established than certainly cell therapy and gene therapies. But we want to really be going after problems and have the right tools in hand to go after those problems. And someday it may in fact require a nucleic acid, or it may require a cell therapy, and we want to be able to have the wherewithal to do that should we want to do that well into the future. So it’s really different. And the type of discovery work that we’re doing here, very few companies do.
“I’ve seen a number of biotechs that start with a discovery engine, target discovery. When they get a few things, that engine is turned off, the people are let go. We really are trying to build — as one of our B-round investors put it — quote: A pharma company, a sort of pharma diversification with the biotech upside.”
9. Orna Therapeutics: The O is circular
This second-gen mRNA player is growing out of some rich soil in Cambridge, MA
↑
CEO: Tom Barnes
CSO: Robert Mabry
Based: Cambridge, MA
Backers: Merck, which dropped its big mRNA alliance with Moderna in vaccines, put up $150 million to partner with Orna, adding $100 million for the last equity round. MPM Capital and BioImpact Capital, an affiliate of MPM, founded the company and put in money on the recent $221 million raise.
The scoop: Like a lot of the CEOs on this list, and every Endpoints 11, Tom Barnes has been there and done that.
Robert Mabry
He was at Millennium when he got a chance to work with John Maraganore on a subsidiary. He did a spinout that became a part of Gene Logic. Then he joined Mark Levin and the crew at Third Rock, where he got involved in startups like Eleven — which he also named.
Barnes likes naming startups.
He grew up inside the ecosystem in the Boston/Cambridge area. And he knows what trial and error lies at the base of so many startups. Failure is built into the equation.
Earlier, Barnes told me that when he got a chance to take the helm of a stealth called Oroboros, he changed the name to Orna, and he waited for the working theory to fail. When he failed at failing, he prepped for the coming-out party.
But win or lose, nothing is ever truly lost in the biotech ecosystem, says Barnes. It just gets recycled in a never-ending loop of reinvention and renewal.
“It’s kind of like a rainforest,” he tells me. “So it’s a true ecosystem. Things grow and die and they fertilize and they come back and in this analogy, people are like carbon atoms. So you can be in a tree. You can be in the air, you can be in the soil, but you’re still a carbon atom. You’re just somewhere moving around.”
And it keeps getting better as it develops and grows.
“The carbon cycle in this analogy has now gone through several times,” Barnes adds. “So the depth of expertise in terms of those who are truly entrepreneurial, straight-up scientists, the venture folks, it’s very, very sophisticated. Furthermore, because something about the way in which it’s become so intense geographically, it’s so crowded together, it has created a sort of Darwinian crucible. So if you want to be successful in this environment, you have to be on top of your game. You have to have great acumen in seeing the early ideas. You have to be able to — whether it’s charisma or connection — pull the right people. You have to create a culture because people can walk back and get a job downstairs, next door.”
This time around, the ecosystem has spawned a startup that was built on the shoulders of the mRNA pioneers. It is literally a second-generation technology, out of the lab of MIT’s Daniel Anderson, one of the many postdocs that came out of Bob Langer’s incredibly influential sphere in Cambridge, with a big assist from Alex Wesselhoeft, now at Orna.
The big idea here is that the mRNA revolution that enriched Moderna and BioNTech could benefit a lot from some refinement.
That will take better lipid nanoparticles and a circular construct that Orna believes should be simpler, easier and less expensive to manufacture than gen 1. Their initial focus is on CAR-T — dubbed isCAR. The lead preclinical drug is ORN-101, an anti-CD19 therapy for lymphoma, with a timeline that points to the clinic in 2024.
If they can keep on failing to fail, Orna has potential to evolve into a leader in the mRNA 2.0 space. If not, all that talent and expertise will be plowed back into the rich Boston/Cambridge ecosystem, looking to do something even better.
10. Rome Therapeutics: A voyage into the dark genome
“People that come to this company, they have to be courageous. They have to be bold. They have to be explorers.”
↑
CEO: Rosana Kapeller
CSO: Dennis Zaller
Based: Cambridge, MA
Backers: The $77 million Series B round was led by new investor Section 32. New investors Sanofi Ventures, Casdin Capital, Andreessen Horowitz and Alexandria Venture Investments came in on the round alongside existing investors: ARCH Ventures, GV and Mass General Brigham Ventures (formerly Partners Innovation Fund).
The scoop: Perhaps it wasn’t a great idea for me to start my interview with Rosana Kapeller by trying to synopsize the science involved in studying the dark genome — the once largely neglected “junkyard” of DNA. Clumsily shoehorning it into a few sentences wasn’t going to work, as you can see from her explanation in response.
Dennis Zaller
“Think about the dark genome as everything that does not encode for the known proteins, okay? And does not encode for the known regulatory elements, like the promoters, the enhancers. Okay, so if you take all that, it’s about 20 to 22% of our genome, that 2% encodes for proteins and about 20% regulates that … whereas the rest of it is called the dark genome.
“Within the dark genome, there are just repetitive sequences. And these repetitive sequences, they may be coding or non-coding. So the repetitive sequences that are coding can code for a variety of proteins that are viral-like. So these repetitive elements are viruses that have integrated into our genome’s re-evolution. So I think that’s another very important concept. They just didn’t appear. They have been integrated into the genome and these coding and non-coding repetitive sequences, some of them encode reverse transcriptase.
“Okay, so we have been calling this endogenous reverse transcriptase, but there are several reverse transcriptases. And we are now focusing on a particular one, which is line-1 reverse transcriptase. And that reverse transcriptase will reverse transcribe itself, or they are the non-coding repetitive RNAs that are derived from viruses, and that is what is the viral mimicry mechanism. Because as these nucleic acids look like viruses, they activate our innate immune system. And interferon is just one biological outcome of that.
“We just talk about interferon as the model, as the way to explain it in a very easy way. And if you think about it, it’s a mechanism that we have evolved to protect us. So when we are in the sun, or we are smoking or whatever, we damaged ourselves. We have to have a way to clear those cells out of our organism. So, that viral mimicry mechanism, by activating the innate immune system, tells the rest of the organism, ‘These cells are sick, come eat them, come get rid of them.’ But if this mechanism goes rogue, then it leads to a variety of diseases, including autoimmune diseases, cancer, neurodegeneration, and also has been implicated with aging in general.”
Okay? Got it.
That’s the simple version, anyway, from the Nimbus vet who founded Rome after a stint as an entrepreneur-in-residence at GV — the patient money in biotech looking for big quests which typically require some awesome computing power to back it up. And Rome is starting out by biting off a couple of fields that are within the preserve of the dark genome: autoimmune disease out front, with a parallel track in oncology.
Here’s Kapeller on the tech:
“Think about it as like the dark matter. Everybody knows it exists, everybody knows it’s important, but nobody can measure it. It’s the same idea of the dark genome. Everybody knew it existed. We actually didn’t know it was important. Like fossils and remnants and maybe providing a structure on the chromatin. But it’s only when the technology enabled us to measure it, to see it, is that we realize how important it is.
So what are the technologies? Next-gen sequencing, long read sequences, RNA-Seq, single cell RNA-Seq. The new algorithms that are derived for machine learning. Before we couldn’t even put these repeats together, because it was like having a puzzle with 100,000 pieces. Everything looked exactly the same, there were no edges. How are you going to map that? How are you going to put these things together? So I think that this is a very important piece, is that our computational tools have evolved to enable us to see and to measure the dark genome.”
And that only became possible in the three years since she launched Rome. Next stop: The clinic. Just don’t ask her to put a precise timeline on it yet.
“We are advancing very rapidly into IND-enabling studies,” she says. “So John, you know me, I’m a drug hunter and I’m extremely pragmatic. I would not start a company just based on blue sky. I am fascinated by the biology and the new technologies, and I have always been this kind of person that was in the interface of technology and biology, drug discovery. But for me, what was key is to get medicines to patients as fast as possible. And I don’t have time to wait 20 years to get there …
“We basically block reverse transcriptase, you block interferon, you have an outcome. With oncology, we’re still studying how these processes are really involved and it’s more complicated because you have the interplay of the tumor and the tumor microenvironment, okay? So I think it’s going to be more akin to an immuno-oncology approach, whereas in autoimmune diseases, it’s very straightforward, very, very directional. And it is incredible.”
Breaking new ground requires starting from scratch on all of this, and that largely means working out all the basics in-house. CROs need not apply for this kind of discovery effort.
“It’s different from Nimbus,” she says, “where I had integrated medicinal chemistry and computational chemistry. Here, I need integrated drug discovery with data sciences. They have to go hand in hand. So I’m building two teams in parallel. One that is the drug discovery, drug hunters, development, etc. And another team that’s very technology-driven to understand and map the drug genome. It’s what I call number 2.0 or 3.0. I think there’s a lot of riches there that we haven’t seen yet.”
Working through the pandemic meant a lot of the work at Rome has been done remotely. But that is largely coming to an end as staffers prep a move to a new facility at 201 Brookline Avenue, in September, in Fenway.
“We’re going to be all together,” says Kapeller happily. You get the sense immediately that this is important to her, to Rome. “And I hope that we’re going to be able to continue building this amazing company that we have started with. The one thing though that I have to say that it’s very important to me to hire the right people. And I think that the people that come to this company, they have to be courageous. They have to be bold. They have to be explorers. This is not for the faint of the heart.”
11. Versanis Bio: Some things never change
Mark Pruzanski learned early that it takes tenacity to make it in biotech
↑
CEO: Mark Pruzanski
CSO: Lloyd Klickstein
Based: New YorkCity
Backers: Joe Jimenez’s Aditum Bio seeded the biotech, which in-licensed bimagrumab from Novartis. Atlas Venture and Medicxi co-led the $70 million Series A financing with support from Aditum Bio.
The scoop: Over the past 20 years, since Mark Pruzanski put together the initial plans for Intercept in his living room in the midst of a market downturn, he’s seen all the good times and all the bad times Nasdaq has had to offer biotech execs.
Lloyd Klickstein
Some things, big things, have changed dramatically over that time. As biotech got bigger, and spread into places like New York where there was little in the way of an ecosystem, the swelling fortunes of the industry fundamentally changed the dynamics of launching a drug developer. There’s much, much more talent on hand, even if you have to compete for it.
But some things haven’t changed.
You still need a level of tenacity that can sustain you and your teams for decades, if necessary.
“Is biotech necessary to drive innovation? If you think about the kinds of leaders, starting with the founders, long term leaders, John (Maraganore) and Barry (Greene) and others at Alnylam, they had several near-death experiences along the way,” says Pruzanski. “They were partnered with Big Pharma companies that gave up on the technology. They never wavered. They believed in it passionately and I think again, that’s a part of the answer. We need leaders like that, risk-takers like that, who have the passion and the stick-to-itiveness, not sure if that’s a word, to really, ultimately succeed.”
This next leg of Pruzanski’s biotech odyssey won’t be quite so long, but that’s because his drug already has a yearslong track record — which abruptly, if temporarily, ground to a halt in 2016 with its failure for a muscle wasting disease. Based on the data they saw at Novartis, though, Joe Jimenez and Mark Fishman at Aditum felt they could get in on the ground floor of a new era in weight management therapeutics, angling ahead with the drug that might shave weight and add some muscle — a distinguishing factor that could offer advantages in a market likely to be dominated for the near term by Eli Lilly’s tirzepatide and Novo Nordisk’s semaglutide, already approved.
Those data turned up around 2019, prompting the ex-Novartis execs to take the plunge.
“As you know well, the US is an obese country,” Pruzanski says. “We’re coming up on close to 50% of the adult population as obese, meaning a BMI north of 30. If you go broader to those who are overweight, BMI 27 and up, it’s a significant majority of the country. And this begets a lot of adverse health sequelae. A recent study showing it at least doubles your per capita healthcare spend on an annual basis and results in an amazing amount of morbidity mortality, not just in the obvious cardio metabolic areas that we’re all familiar with, but a number of different cancers.”
Jean-Francois Formela
One of the not-so-subtle messages about the Versanis story — like others in the Endpoints 11 — is that you need to play nice in the sandbox. Those people you start out with at low level jobs, or in short-lived startups, will come around later with their own networks of researchers and investors and pharma connections. And they can make the difference between success or failure. If not this year or decade, then in the next.
That message will likely be particularly acute for Pruzanski, who got his first advice on biotech as a medical student, when he reached out to Atlas’s Jean-Francois Formela. Formela is a key backer at Versanis, and finally, after all this time, they’re working hand in hand. In addition, industry stalwart Maraganore is on his board, and ready with his own stubborn advice.
John Maraganore
Now it’s Pruzanski’s turn to lend his advice. And he’s happy to do it.
“I have experienced it where I’ve gotten a hug from someone who’s taking a drug that I spent 15 years getting to market and believing in and thanking me for saving their lives,” he says. “Now that’s their perception. But there’s honestly nothing more gratifying than that feeling. And so I tell anyone who’s interested, absolutely go for it. The industry needs more and more talent. It takes a long time to get up to speed and to really develop yourself and frankly, there’s a lot of failure along the way that anyone in our business does experience. So, you’ve got to brace yourself for that and take the long view, but I encourage people, young people, to get in.”
Former Project Veritas & O’Keefe Media Group operative and Pfizer formulation analyst scientist Justin Leslie revealed previously unpublished recordings showing Pfizer’s top vaccine researchers discussing major concerns surrounding COVID-19 vaccines. Leslie delivered these recordings to Veritas in late 2021, but they were never published:
Principal scientist at Pfizer, Kanwall Gill in 2021:
“We had no idea how it’s going to look like. MRNA vaccines have been there for 50 years, but nothing went to clinical trial because MRNA have been known to have side effects.”
Featured in Leslie’s footage is Kanwal Gill, a principal scientist at Pfizer. Gill was weary of MRNA technology given its long research history yet lack of approved commercial products. She called the vaccines “sneaky,” suggesting latent side effects could emerge in time.
Gill goes on to illustrate how the vaccine formulation process was dramatically rushed under the FDA’s Emergency Use Authorization and adds that profit incentives likely played a role:
Pfizer's principal scientist in 2021:
“It takes 10 year for a vaccine to come out. It takes years of observations... we are doing everything at the same time."
"It’s going to affect my heart, and I’m going to die. And nobody’s talking about that."
Leslie recorded another colleague, Pfizer’s pharmaceutical formulation scientist Ramin Darvari, who raised the since-validated concern that repeat booster intake could damage the cardiovascular system:
Pfizer's pharmaceutical formulation scientist, Ramin Darvari, in 2021:
“They’re engineering it specifically for me to take the next one, so increasing my consumption."
“It’s going to affect my heart, and I’m going to die. And nobody’s talking about that.”
None of these claims will be shocking to hear in 2024, but it is telling that high-level Pfizer researchers were discussing these topics in private while the company assured the public of “no serious safety concerns” upon the jab’s release:
Vaccine for Children is a Different Formulation
Leslie sent me a little-known FDA-Pfizer conference — a 7-hour Zoom meeting published in tandem with the approval of the vaccine for 5 – 11 year-olds — during which Pfizer’s vice presidents of vaccine research and development, Nicholas Warne and William Gruber, discussed a last-minute change to the vaccine’s “buffer” — from “PBS” to “Tris” — to improve its shelf life. For about 30 seconds of these 7 hours, Gruber acknowledged that the new formula was NOT the one used in clinical trials (emphasis mine):
“The studies were done using the same volume… but contained the PBS buffer. We obviously had extensive consultations with the FDA and it was determined that the clinical studies were not required because, again, the LNP and the MRNA are the same and the behavior — in terms of reactogenicity and efficacy — are expected to be the same.”
According to Leslie, the tweaked “buffer” dramatically changed the temperature needed for storage: “Before they changed this last step of the formulation, the formula was to be kept at -80 degrees Celsius. After they changed the last step, we kept them at 2 to 8 degrees celsius,” Leslie told me.
The claims are backed up in the referenced video presentation:
I’m no vaccinologist but an 80-degree temperature delta — and a 5x shelf-life in a warmer climate — seems like a significant change that might warrant clinical trials before commercial release.
Despite this information technically being public, there has been virtually no media scrutiny or even coverage — and in fact, most were told the vaccine for children was the same formula but just a smaller dose — which is perhaps due to a combination of the information being buried within a 7-hour jargon-filled presentation and our media being totally dysfunctional.
Bohemian Grove?
Leslie’s 2-hour long documentary on his experience at both Pfizer and O’Keefe’s companies concludes on an interesting note: James O’Keefe attended an outing at the Bohemian Grove.
Leslie offers this photo of James’ Bohemian Grove “GATE” slip as evidence, left on his work desk atop a copy of his book, “American Muckraker”:
My thoughts on the Bohemian Grove: my good friend’s dad was its general manager for several decades. From what I have gathered through that connection, the Bohemian Grove is not some version of the Illuminati, at least not in the institutional sense.
Do powerful elites hangout there? Absolutely. Do they discuss their plans for the world while hanging out there? I’m sure it has happened. Do they have a weird ritual with a giant owl? Yep, Alex Jones showed that to the world.
My perspective is based on conversations with my friend and my belief that his father is not lying to him. I could be wrong and am open to evidence — like if boxer Ryan Garcia decides to produce evidence regarding his rape claims — and I do find it a bit strange the club would invite O’Keefe who is notorious for covertly filming, but Occam’s razor would lead me to believe the club is — as it was under my friend’s dad — run by boomer conservatives the extent of whose politics include disliking wokeness, immigration, and Biden (common subjects of O’Keefe’s work).
Therefore, I don’t find O’Keefe’s visit to the club indicative that he is some sort of Operation Mockingbird asset as Leslie tries to depict (however Mockingbird is a 100% legitimate conspiracy). I have also met James several times and even came close to joining OMG. While I disagreed with James on the significance of many of his stories — finding some to be overhyped and showy — I never doubted his conviction in them.
As for why Leslie’s story was squashed… all my sources told me it was to avoid jail time for Veritas executives.
Feel free to watch Leslie’s full documentary here and decide for yourself.
Fun fact — Justin Leslie was also the operative behind this mega-viral Project Veritas story where Pfizer’s director of R&D claimed the company was privately mutating COVID-19 behind closed doors:
BREAKING: @Pfizer Exploring "Mutating" COVID-19 Virus For New Vaccines
"Don't tell anyone this...There is a risk...have to be very controlled to make sure this virus you mutate doesn't create something...the way that the virus started in Wuhan, to be honest."#DirectedEvolutionpic.twitter.com/xaRvlD5qTo
“[…] our findings support the hypothesis that the intrauterine environment, particularly essential and non-essential metals, affect epigenetic aging biomarkers across the life course.”
Credit: 2024 Bozack et al.
“[…] our findings support the hypothesis that the intrauterine environment, particularly essential and non-essential metals, affect epigenetic aging biomarkers across the life course.”
BUFFALO, NY- March 12, 2024 – A new research paper was published inAging (listed by MEDLINE/PubMed as “Aging (Albany NY)” and “Aging-US” by Web of Science) Volume 16, Issue 4, entitled, “Associations of prenatal one-carbon metabolism nutrients and metals with epigenetic aging biomarkers at birth and in childhood in a US cohort.”
Epigenetic gestational age acceleration (EGAA) at birth and epigenetic age acceleration (EAA) in childhood may be biomarkers of the intrauterine environment. In this new study, researchers Anne K. Bozack, Sheryl L. Rifas-Shiman, Andrea A. Baccarelli, Robert O. Wright, Diane R. Gold, Emily Oken, Marie-France Hivert, and Andres Cardenas from Stanford University School of Medicine, Harvard Medical School, Harvard T.H. Chan School of Public Health, Columbia University, and Icahn School of Medicine at Mount Sinai investigated the extent to which first-trimester folate, B12, 5 essential and 7 non-essential metals in maternal circulation are associated with EGAA and EAA in early life.
“[…] we hypothesized that OCM [one-carbon metabolism] nutrients and essential metals would be positively associated with EGAA and non-essential metals would be negatively associated with EGAA. We also investigated nonlinear associations and associations with mixtures of micronutrients and metals.”
Bohlin EGAA and Horvath pan-tissue and skin and blood EAA were calculated using DNA methylation measured in cord blood (N=351) and mid-childhood blood (N=326; median age = 7.7 years) in the Project Viva pre-birth cohort. A one standard deviation increase in individual essential metals (copper, manganese, and zinc) was associated with 0.94-1.2 weeks lower Horvath EAA at birth, and patterns of exposures identified by exploratory factor analysis suggested that a common source of essential metals was associated with Horvath EAA. The researchers also observed evidence of nonlinear associations of zinc with Bohlin EGAA, magnesium and lead with Horvath EAA, and cesium with skin and blood EAA at birth. Overall, associations at birth did not persist in mid-childhood; however, arsenic was associated with greater EAA at birth and in childhood.
“Prenatal metals, including essential metals and arsenic, are associated with epigenetic aging in early life, which might be associated with future health.”
Read the full paper: DOI:https://doi.org/10.18632/aging.205602
Corresponding Author: Andres Cardenas
Corresponding Email:andres.cardenas@stanford.edu
Keywords: epigenetic age acceleration, metals, folate, B12, prenatal exposures
Click here to sign up for free Altmetric alerts about this article.
About Aging:
Launched in 2009, Aging publishes papers of general interest and biological significance in all fields of aging research and age-related diseases, including cancer—and now, with a special focus on COVID-19 vulnerability as an age-dependent syndrome. Topics in Aging go beyond traditional gerontology, including, but not limited to, cellular and molecular biology, human age-related diseases, pathology in model organisms, signal transduction pathways (e.g., p53, sirtuins, and PI-3K/AKT/mTOR, among others), and approaches to modulating these signaling pathways.
Please visit our website at www.Aging-US.com and connect with us:
National insurance, income tax, VAT, capital gains tax, inheritance tax… it’s easy to get confused about the many different ways we contribute to the cost of running the country. The budget announcement is the key time each year when the government shares its financial plans with us all, and announces changes that may make a tangible difference to what you pay.
But you’ll likely be hearing a lot more about taxes in the coming months – promises to cut or raise them are an easy win (or lose) for politicians in an election year. We may even get at least one “mini-budget”.
If you’ve recently entered the workforce or the housing market, you may still be wrapping your mind around all of these terms. Here is what you need to know about the different types of taxes and how they affect you.
The UK broadly uses three ways to collect tax:
1. When you earn money
If you are an employee or own a business, taxes are deducted from your salary or profits you make. For most people, this happens in two ways: income tax, and national insurance contributions (or NICs).
If you are self-employed, you will have to pay your taxes via an annual tax return assessment. You might also have to pay taxes this way for interest you earn on savings, dividends (distribution of profits from a company or shares you own) received and most other forms of income not taxed before you get it.
VAT and excise duties are taxes on most goods and services you buy, with some exceptions like books and children’s clothing. About 20% of the total tax collected is VAT.
3. Taxes on wealth and assets
These are mainly taxes on the money you earn if you sell assets (like property or stocks) for more than you bought them for, or when you pass on assets in an inheritance. In the latter case in the UK, the recipient doesn’t pay this, it is the estate paying it out that must cover this if due. These taxes contribute only about 3% to the total tax collected.
You also likely have to pay council tax, which is set by the council you live in based on the value of your house or flat. It is paid by the user of the property, no matter if you own or rent. If you are a full-time student or on some apprenticeship schemes, you may get a deduction or not have to pay council tax at all.
This article is part of Quarter Life, a series about issues affecting those of us in our 20s and 30s. From the challenges of beginning a career and taking care of our mental health, to the excitement of starting a family, adopting a pet or just making friends as an adult. The articles in this series explore the questions and bring answers as we navigate this turbulent period of life.
Put together, these totalled almost £790 billion in 2022-23, which the government spends on public services such as the NHS, schools and social care. The government collects taxes from all sources and sets its spending plans accordingly, borrowing to make up any difference between the two.
Income tax
The amount of income tax you pay is determined by where your income sits in a series of “bands” set by the government. Almost everyone is entitled to a “personal allowance”, currently £12,570, which you can earn without needing to pay any income tax.
You then pay 20% in tax on each pound of income you earn (across all sources) from £12,570-£50,270. You pay 40% on each extra pound up to £125,140 and 45% over this. If you earn more than £100,000, the personal allowance (amount of untaxed income) starts to decrease.
If you are self-employed, the same rates apply to you. You just don’t have an employer to take this off your salary each month. Instead, you have to make sure you have enough money at the end of the year to pay this directly to the government.
The government can increase the threshold limits to adjust for inflation. This tries to ensure any wage rise you get in response to higher prices doesn’t lead to you having to pay a higher tax rate. However, the government announced in 2021 that they would freeze these thresholds until 2026 (extended now to 2028), arguing that it would help repay the costs of the pandemic.
Given wages are now rising for many to help with the cost of living crisis, this means many people will pay more income tax this coming year than they did before. This is sometimes referred to as “fiscal drag” – where lower earners are “dragged” into paying higher tax rates, or being taxed on more of their income.
National insurance
National insurance contributions (NICs) are a second “tax” you pay on your income – or to be precise, on your earned income (your salary). You don’t pay this on some forms of income, including savings or dividends, and you also don’t pay it once you reach state retirement age (currently 66).
While Jeremy Hunt, the current chancellor of the exchequer, didn’t adjust income tax meaningfully in this year’s budget, he did announce a cut to NICs. This was a surprise to many, as we had already seen rates fall from 12% to 10% on incomes higher than £242/week in January. It will now fall again to 8% from April.
While this is charged separately to income tax, in reality it all just goes into one pot with other taxes. Some, including the chancellor, say it is time to merge these two deductions and make this simpler for everyone. In his budget speech this year, Hunt said he’d like to see this tax go entirely. He thinks this isn’t fair on those who have to pay it, as it is only charged on some forms of income and on some workers.
I wouldn’t hold my breath for this to happen however, and even if it did, there are huge sums linked to NICs (nearly £180bn last year) so it would almost certainly have to be collected from elsewhere (such as via an increase in income taxes, or a lot more borrowing) to make sure the government could still balance its books.
There are likely to be further tweaks to the UK’s tax system soon, perhaps by the current government before the election – and almost certainly if there is a change of government.
Wealth taxes may be in line for a change. In the budget, the chancellor reduced capital gains taxes on sales of assets such as second properties (from 28% to 24%). These types of taxes provide only a limited amount of money to the government, as quite high thresholds apply for inheritance tax (up to £1 million if you are passing on a family home).
There are calls from many quarters though to look again at these types of taxes. Wealth inequality (the differences between total wealth held by the richest compared to the poorest) in the UK is very high (much higher than income inequality) and rising.
But how to do this effectively is a matter of much debate. A recent study suggested a one-off tax on total wealth held over a certain threshold might work. But wealth taxes are challenging to make work in practice, and both main political parties have already said this isn’t an option they are considering currently.
Andy Lymer and his colleagues at the Centre for Personal Financial Wellbeing at Aston University currently or have recently received funding for their research work from a variety of funding bodies including the UK's Money and Pension Service, the Aviva Foundation, Fair4All Finance, NEST Insight, the Gambling Commission, Vivid Housing and the ESRC, amongst others.
We use cookies on our website to give you the most relevant experience by remembering your preferences and repeat visits. By clicking “Accept”, you consent to the use of ALL the cookies.
This website uses cookies to improve your experience while you navigate through the website. Out of these, the cookies that are categorized as necessary are stored on your browser as they are essential for the working of basic functionalities of the website. We also use third-party cookies that help us analyze and understand how you use this website. These cookies will be stored in your browser only with your consent. You also have the option to opt-out of these cookies. But opting out of some of these cookies may affect your browsing experience.
Necessary cookies are absolutely essential for the website to function properly. These cookies ensure basic functionalities and security features of the website, anonymously.
Cookie
Duration
Description
cookielawinfo-checbox-analytics
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Analytics".
cookielawinfo-checbox-functional
11 months
The cookie is set by GDPR cookie consent to record the user consent for the cookies in the category "Functional".
cookielawinfo-checbox-others
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Other.
cookielawinfo-checkbox-necessary
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookies is used to store the user consent for the cookies in the category "Necessary".
cookielawinfo-checkbox-performance
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Performance".
viewed_cookie_policy
11 months
The cookie is set by the GDPR Cookie Consent plugin and is used to store whether or not user has consented to the use of cookies. It does not store any personal data.
Functional cookies help to perform certain functionalities like sharing the content of the website on social media platforms, collect feedbacks, and other third-party features.
Performance cookies are used to understand and analyze the key performance indexes of the website which helps in delivering a better user experience for the visitors.
Analytical cookies are used to understand how visitors interact with the website. These cookies help provide information on metrics the number of visitors, bounce rate, traffic source, etc.
Advertisement cookies are used to provide visitors with relevant ads and marketing campaigns. These cookies track visitors across websites and collect information to provide customized ads.














































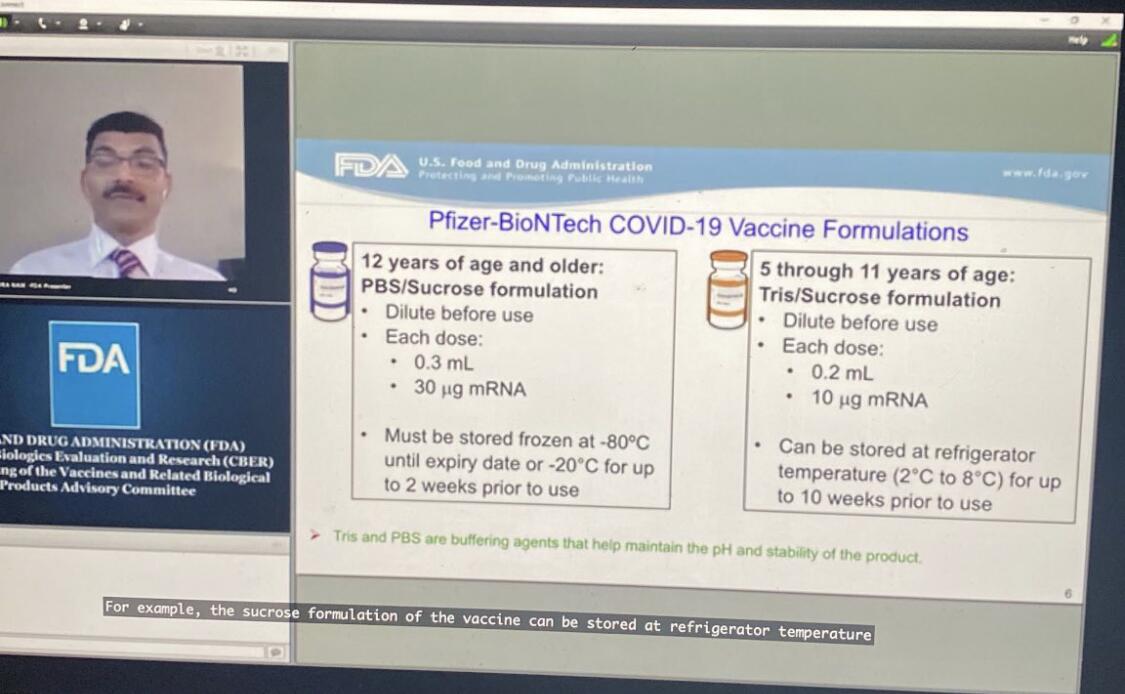

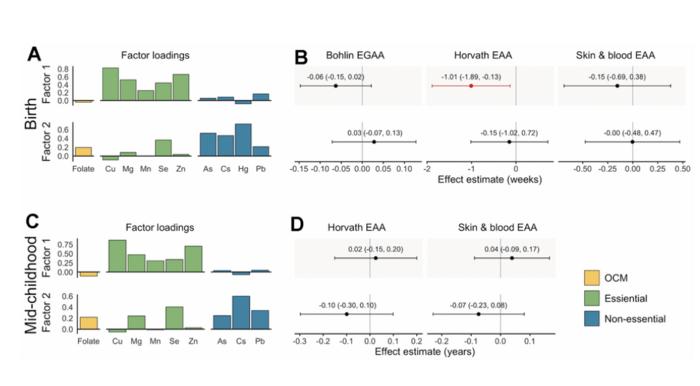








































{kind=link}