What was the basis of panic that led the lights to darken on civilization?
The most important date here might be March 11, 2020. That’s when Congress itself flew into an unwarranted panic, and acquiesced to a lockdown at the urging of the “experts.”
State governors followed one by one, with few exceptions, and the rest of the world joined the lockdown frenzy.
In February, people were aching to know the answer to the following.
Would this “novel virus” have familiar patterns we associate with the flu, seasonal colds, and other predictable and manageable pathogens? Or would this be something entirely different, unprecedented in our lifetimes, terrifying, and universally deadly?
Crucial in this stage was public-health messaging. In previous pandemics from post-1918 throughout the 20th century, the central messaging was to stay calm, go to the doctor if you feel sick, avoid deliberately infecting others, and otherwise trust the systems in place and keep society functioning. This was long considered responsible public-health messaging, and this was pretty much where we stood throughout most of January and February, when publications regardless of their political outlook maintained sobriety and rationality.
Something dramatically changed this time. They pushed panic, tapping into a primal fear of disease. The reality of pandemic, as it turns out, has been familiar. The severity of its impact has been radically disparate across demographics, hitting mainly the elderly and infirm with 40% of deaths tracing to long-term care facilities with an average age of death nearly equal to the average lifespan. It is regionally migratory. It follows a seasonal pattern from pandemic to its endemic equilibrium.
What has been different has been the messaging that has almost universally been structured to create public frenzy, from the New York Times’s February 28 urge to “go medieval” to Salon’s latest demand that we panic even more.
My own sense of impending doom began on March 6 with the cancellation of South by Southwest in Austin, Texas, an action of the mayor alone, and completely without modern precedent. I wrote about it on March 8. Four days later, President Trump gave a nationwide address that ended with a shocking announcement that all flights from Europe would be stopped to keep the coronavirus out even though the virus had been here since January. The next day, on March 13, the administration issued what amounted to a shutdown plan for the nation.
Our author’s thesis was that the wild overreaction and unprecedented lockdowns of life began with what was a terminological mixup that led to a misplacement of a decimal point in a report from the National Institutes of Health.
It was a seemingly small error but it provided the basis on which Anthony Fauci testified at the House Oversight and Reform Committee about the seriousness of novel coronavirus spreading across the globe.
Here is the video in question. As you watch, you will note the seeming precision of data that actually masks a huge problem. He obscures the huge difference between the infection fatality rate, the case fatality rate, and the overall death rate. Nowhere does he mention survival rates. Not one person present pushed back on his claims. In the blizzard of data, he finally summarizes in a way that terrified everyone. Covid, he said, is “10 times more lethal than the seasonal flu.”
Even apart from that prediction, his entire demeanor was: this is entirely new, very deadly, and unbearably unmanageable without extreme measures. Fauci’s implicit message to Congress and the American people was that it is time to panic.
Fauci was claiming what in fact he could not know, conflating two distinct data sets, and extrapolating in ways that allowed him to make a completely unsupported claim that very obviously turned out to be false. Two years ago, 61,000 Americans of all ages died of flu, exclusive of other ailments.
If you incorrectly impose on that a “case fatality rate” of 0.1% and extrapolate to Covid infections, you end up with at least 800,000 deaths from Covid alone – not “with” or “involving” Covid as the CDC classifies deaths today (that alone represents a big change). This is a scary prediction at the time; it seemed to add weight to the estimates out of the Imperial College of London that 2.2 million people would die without locking down. This testimony led a whole generation of lawmakers to believe that none of the traditional medical measures could or would work. There is no comparing this with the flu or any respiratory illness. This was the Other that justified a once-in-many-generations national emergency that required an end to our way of life.
The trouble is that the whole claim was based on a terminological misstatement that fed a basic math error. As Brown explains:
Sampling bias in coronavirus mortality calculations led to a 10-fold increased mortality overestimation in March 11, 2020, US Congressional testimony. This bias most likely followed from information bias due to misclassifying a seasonal influenza IFR as a CFR, evident in a NEJM.org editorial. Evidence from the WHO confirmed that the approximate CFR of the coronavirus is generally no higher than that of seasonal influenza. By early May 2020, mortality levels from COVID-19 were considerably below predicted overestimations, a result that the public attributed to successful mitigating measures to contain the spread of the novel coronavirus.
Let’s follow Brown here as he takes the reader through the crucial differences between the IFR and the CFR. IFRs from samples across the population “include undiagnosed, asymptomatic, and mild infections.” To calculate the average IFR across the population, you do randomized samples to judge its prevalence. The results are inclusive of cases – what we used to call actual “sick” people – but extend to people who merely carry traces of the dead virus but are in no substantial danger of passing it onward or experiencing any severe outcomes. Cases, on the other hand, “are based exclusively on relatively smaller groups of moderately to severely ill diagnosed cases at the beginning of an outbreak.” The CFR is a smaller group. Brown provides the following graphic to show how epidemiology has long considered the difference.
Based on this graphic alone, you can see why it becomes crucial to keep these terms straight.
The CFR is higher; IFR is lower; the crude mortality rate is lower still.
The CFR measures severity; the IFR measures prevalence.
Those are the two general issues one needs to know to assess whether and to what extent a virus outbreak is mild, moderate, serious, or severe. This matters due to the long-observed evolved reality of respiratory viruses: there is a trade off between the forces. The more severe the virus, the quicker it burns itself out. The milder (and “smarter”) it is, the more it can spread. To mix up severity and prevalence is to make a mess of all the important categories that infectious disease specialists use to assess the social impact of a new virus.
Moreover, if you are going to compare how severe a pandemic is, you have to compare apples to apples, which means at the very minimum that we must be careful to distinguish apples from oranges from pears. That is precisely what the early messaging surrounding the coronavirus did not do.
Cases are not deaths; even more crucially, cases in a traditional sense mean that people are actually sick, not merely that they have been tested positive by a PCR test. Adding to the confusion, most data sources on Covid today use the term “cases” to identify any positive test, with or without symptoms, when the correct word would be “infections.” Further, the PCR test itself presents its own problems. As Brown notes, “A serious limitation of RT-PCR testing is that nucleic acid detection is not capable of determining the difference between infective and noninfective viruses.” The widespread use of the PCR test has made its own contribution to blurring all these crucial distinctions.
Now consider an extraordinary article from the New England Journal of Medicine that appeared on February 28, with Anthony Fauci as the co-author. The import of the piece was to claim that Covid and flu are quite similar in severity.
“The overall clinical consequences of Covid-19 may ultimately be more akin to those of a severe seasonal influenza (which has a case fatality rate of approximately 0.1%) or a pandemic influenza (similar to those in 1957 and 1968) rather than a disease similar to SARS or MERS, which have had case fatality rates of 9 to 10% and 36%, respectively.”
What matters here is not the prediction as such but the switching of the word infection with case: the flu has “a case fatality rate of approximately 0.1%.” This was incorrect even at the time of writing. You can call it a misprint or sloppy or downright duplicitous. Regardless, even the World Health Organization had identified the 0.1% figure as the flu’s infection fatality rate. If you assume one symptomatic confirmed case for every infection (or what is now confusingly called “cumulative cases”), the error could be a misplace decimal: 0.01% not 0.1%. Regardless, Fauci’s article directly contradicted the WHO, and ran counter to everything that was already then known. But his CFR claim about flu is precisely what led him to claim in front of the Congressional committee that Covid would be deadly in ways that defy all experience of this generation.
Brown further explains:
As the campaign to mitigate coronavirus transmission was implemented from March into May, 2020, expected coronavirus mortality totals in the United States appeared much lower than the overestimation reported in Congressional testimony on March 11. Compared with the most recent season of severe influenza A (H3N2) in 2017-2018,with 80,000 US deaths reported by CDC officials, US coronavirus mortality totals had just reached 80,000 on May 9, 2020. By then, relative to the 2017-2018 influenza, it was clear that the coronavirus mortality total for the season would be nowhere near 800,000 deaths inferred from the 10-fold mortality overestimation reported to Congress. Even after adjusting for the effect of successful mitigation measures that may have slowed down the rate of coronavirus transmission, it seems unlikely that so many deaths were completely eliminated by a nonpharmaceutical intervention such as social distancing, which was only intended to contain infection transmission, not suppress infections and related fatalities. Also in early May, 2020, a New York State survey of 1,269 COVID-19 patients recently admitted to 113 hospitals found that most of the patients had been following shelter-in-place orders for 6 wk, which raised state officials’ suspicions about social distancing effectiveness. Still, polls showed the public credited social distancing and other mitigation measures for reducing predicted COVID-19 deaths, and for keeping people safe from the coronavirus.
As of this writing, however, deaths “involving” or “with” Covid has passed 300,000, which while less than half as high as what Congress heard they would be on March 11, is still quite high, provided these deaths have not been broadly misclassified. However, on March 24, the CDC made an announcement of serious significance. It would now calculate coronavirus mortality by including “probable” and “likely” deaths in the International Classification of Diseases code (ICD).
This became an invitation to misclassification. People who otherwise would have previously been classified as having heart disease or some other comorbidity could now be classified as Covid. This also included a financial incentive to do just that. For this reason, when the CDC announced that “for 6% of the deaths, Covid-19 was the only cause mentioned,” it came as a shock to people. What that means is that 94% of the deaths attributed to Covid were associated with additional comorbidities that prevented the immune system from fighting off the virus.
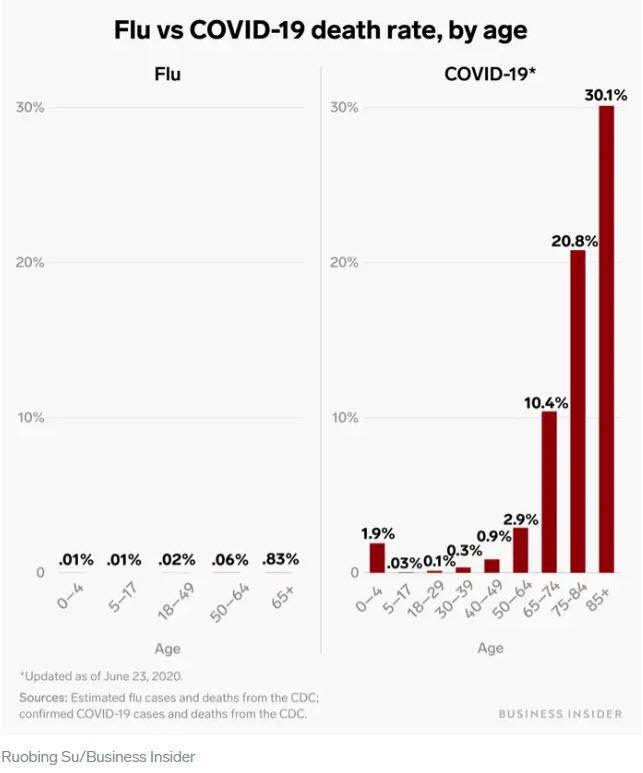
Following the March 11 Fauci testimony, in which he conflated IFR and CFR, the national media went wild with Covid and flu comparison. The following article, for example, blew up from BusinessInsider in June: “The coronavirus death rate in the US is almost 50 times higher than that of the flu. See how they compare by age bracket.” If you look carefully at the charts, you can see something fishy: they calculated infection fatality rate for flu against the case fatality rate for Covid. That necessarily generates a wild overestimate for Covid deaths. The charts are terrifying – and have nothing to do with reality.
Let’s hop forward from the testimony days to one month later when full-scale panic had already hit the U.S. Speaking at a White House press conference, Fauci then made a claim that strains credulity at every level. He said at a White House press briefing that the stringencies and “social distancing” could not and would not be relaxed until there are no “no new cases, no deaths.” Such a thing has happened only once in the history of viruses: smallpox. From the first experiments with inoculation to the final eradication took some 250 years. And yet here we have Fauci explaining that life could not be normal and functioning again until this widespread virus, relatively mild for 95% of the population, was completely eradicated from the planet!
And now we have the vaccine, and plenty of questions remaining about it, such as why non-vulnerable populations would prefer to take it over gaining the exposure necessary for naturally acquired immunity. Asking such a basic question is very close to being tabooed, even as lawmakers and other institutions are toying with the idea of making it mandatory. Even then, many of the lockdown advocates from earlier this year are saying that it will not enable us to go back to normal, to take off the masks, to go to the movies, or travel again. This is precisely the belief you might expect from a crowd that participated in what John Iaonnidis called a “one-in-a-century evidence fiasco” and are desperately trying to dig themselves out of losing every bit of scientific credibility.
Whether Brown is correct that the whole panic truly does trace to a brain flakeout on the part of Fauci – or even perhaps a deliberate “noble lie” to deceive the public into accepting the unacceptable – it hardly matters. The problem we face now is a huge tangle over terminology such that “infections” that could include as many as 90% false positives (according to the NYT) are called cases, while the once-distinct condition called cases which used to indicate actually being sick no longer has any precise meaning. The cacophony of statistical confusion here truly boggles the mind.
In the midst of all of this, the CDC itself finally updated its own estimates of the infection fatality rate of Covid-19. The CDC wisely took account of the huge demographic stratification of severe outcomes. There is not one rate that applies to the whole population or to any particular individual. There are only backward looking estimates of outcomes. They are all follows:
0.003% for 0-19 years
0.02% for 20-49 years
0.5% for 50-69 years
5.4% for 70+ years
Flipping the data to state it by survival rate by age:
99.997% for 0-19 years
99.98% for 20-49 years
99.5% for 50-69 years
94.6% for 70+ years
John Ioannidis sums up the disparity by age with the following infection fatality rate for people under the age of 70: 0.05%. This conclusion has been peer-reviewed and published by the World Health Organization.
How does this compare with the flu? We do not really know. As science journalist Shin Jie Yong has written, “There seems to be no data on age-specific IFR of the seasonal flu.” What this means is that crucial testimony of Fauci from March 11, in which he casually predicted based on bad numbers, that Covid would be ten times worse than the flu, can neither be confirmed or denied based on age-specific severe outcomes.
However, we can assemble the data based on years of lost life. Consider the long-term view over the future course of existing lifetimes. JusttheFacts reports:
If 500,000 Covid-19 deaths ultimately [in the future] occur in the United States—or more than twice the level of a prominent projection—the disease will rob about 6.8 million years of life from all Americans who were alive at the outset of 2020.
In contrast:
* the flu will rob them of about 35 million years.
* suicides will rob them of 132 million years.
* accidents will rob them of 409 million years.
As testing has expanded dramatically throughout the population, the estimated infection fatality rate of Covid will fall further. Thus can we observe a chart of “cases” (actually positive tests) all over the world and compare it with severe outcomes and see something remarkable that should make every living person fundamentally question why they decided to shut down the world and wreck billions of lives.
Another statistic that bears repeating, Covid – based on infections vs deaths – has close to a 99.9% survival rate. Imagine how the world would have been different had Fauci told that to the Congress on that fateful day of March 11. Or what if Fauci had revealed that the average age of death from Covid would almost equal the average lifespan in the US and exceed it in most parts of the world? People present might have wondered why they were holding hearings at all.
All these categories of data placement carry with them the danger of creating an illusion of control. Viruses do not come with little gears inside them with these rates. Human beings collect data and create them, and not one of them (whether IFR, CFR, infection rates, mortality rates, survival rates) pertains infallibly to any single individual. Our response to a virus is contingent on our own health, age, cross immunities, T cell memory, and a thousand other factors that no politician controls.
What we know is that a terminological confusion, a misplaced decimal point, a one-word error in data description, and a massive amount of arrogant presumptions about how to control a virus set in motion a series of events that turned our great and prosperous country into a disaster of confusion, demoralization, foregone medical services, closed businesses, wrecked arts and education, and long bread lines. The lockdowners who created this appalling disaster, the people who turned our trust into betrayal and a blizzard of statistical baloney, need to look at the science and data as they stand and come clean.
Chronic stress and inflammation linked to societal and environmental impacts in new study
From anxiety about the state of the world to ongoing waves of Covid-19, the stresses we face can seem relentless and even overwhelming. Worse, these stressors…
From anxiety about the state of the world to ongoing waves of Covid-19, the stresses we face can seem relentless and even overwhelming. Worse, these stressors can cause chronic inflammation in our bodies. Chronic inflammation is linked to serious conditions such as cardiovascular disease and cancer – and may also affect our thinking and behavior.
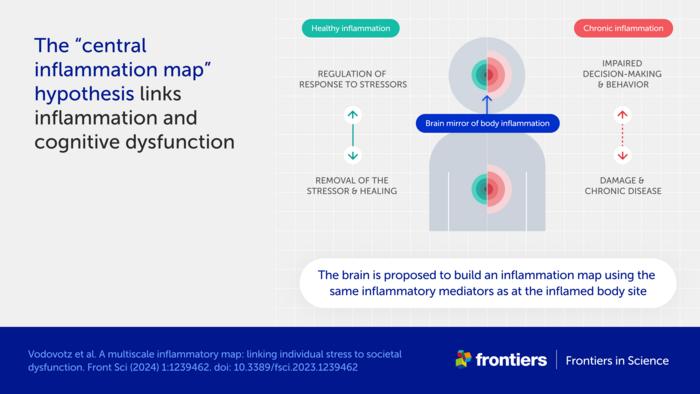
Credit: Image: Vodovotz et al/Frontiers
From anxiety about the state of the world to ongoing waves of Covid-19, the stresses we face can seem relentless and even overwhelming. Worse, these stressors can cause chronic inflammation in our bodies. Chronic inflammation is linked to serious conditions such as cardiovascular disease and cancer – and may also affect our thinking and behavior.
A new hypothesis published in Frontiers in Science suggests the negative impacts may extend far further.
“We propose that stress, inflammation, and consequently impaired cognition in individuals can scale up to communities and populations,” explained lead author Prof Yoram Vodovotz of the University of Pittsburgh, USA.
“This could affect the decision-making and behavior of entire societies, impair our cognitive ability to address complex issues like climate change, social unrest, and infectious disease – and ultimately lead to a self-sustaining cycle of societal dysfunction and environmental degradation,” he added.
Bodily inflammation ‘mapped’ in the brain
One central premise to the hypothesis is an association between chronic inflammation and cognitive dysfunction.
“The cause of this well-known phenomenon is not currently known,” said Vodovotz. “We propose a mechanism, which we call the ‘central inflammation map’.”
The authors’ novel idea is that the brain creates its own copy of bodily inflammation. Normally, this inflammation map allows the brain to manage the inflammatory response and promote healing.
When inflammation is high or chronic, however, the response goes awry and can damage healthy tissues and organs. The authors suggest the inflammation map could similarly harm the brain and impair cognition, emotion, and behavior.
Accelerated spread of stress and inflammation online
A second premise is the spread of chronic inflammation from individuals to populations.
“While inflammation is not contagious per se, it could still spread via the transmission of stress among people,” explained Vodovotz.
The authors further suggest that stress is being transmitted faster than ever before, through social media and other digital communications.
“People are constantly bombarded with high levels of distressing information, be it the news, negative online comments, or a feeling of inadequacy when viewing social media feeds,” said Vodovotz. “We hypothesize that this new dimension of human experience, from which it is difficult to escape, is driving stress, chronic inflammation, and cognitive impairment across global societies.”
Inflammation as a driver of social and planetary disruption
These ideas shift our view of inflammation as a biological process restricted to an individual. Instead, the authors see it as a multiscale process linking molecular, cellular, and physiological interactions in each of us to altered decision-making and behavior in populations – and ultimately to large-scale societal and environmental impacts.
“Stress-impaired judgment could explain the chaotic and counter-intuitive responses of large parts of the global population to stressful events such as climate change and the Covid-19 pandemic,” explained Vodovotz.
“An inability to address these and other stressors may propagate a self-fulfilling sense of pervasive danger, causing further stress, inflammation, and impaired cognition in a runaway, positive feedback loop,” he added.
The fact that current levels of global stress have not led to widespread societal disorder could indicate an equally strong stabilizing effect from “controllers” such as trust in laws, science, and multinational organizations like the United Nations.
“However, societal norms and institutions are increasingly being questioned, at times rightly so as relics of a foregone era,” said Prof Paul Verschure of Radboud University, the Netherlands, and a co-author of the article. “The challenge today is how we can ward off a new adversarial era of instability due to global stress caused by a multi-scale combination of geopolitical fragmentation, conflicts, and ecological collapse amplified by existential angst, cognitive overload, and runaway disinformation.”
Reducing social media exposure as part of the solution
The authors developed a mathematical model to test their ideas and explore ways to reduce stress and build resilience.
“Preliminary results highlight the need for interventions at multiple levels and scales,” commented co-author Prof Julia Arciero of Indiana University, USA.
“While anti-inflammatory drugs are sometimes used to treat medical conditions associated with inflammation, we do not believe these are the whole answer for individuals,” said Dr David Katz, co-author and a specialist in preventive and lifestyle medicine based in the US. “Lifestyle changes such as healthy nutrition, exercise, and reducing exposure to stressful online content could also be important.”
“The dawning new era of precision and personalized therapeutics could also offer enormous potential,” he added.
At the societal level, the authors suggest creating calm public spaces and providing education on the norms and institutions that keep our societies stable and functioning.
“While our ‘inflammation map’ hypothesis and corresponding mathematical model are a start, a coordinated and interdisciplinary research effort is needed to define interventions that would improve the lives of individuals and the resilience of communities to stress. We hope our article stimulates scientists around the world to take up this challenge,” Vodovotz concluded.
The article is part of the Frontiers in Science multimedia article hub ‘A multiscale map of inflammatory stress’. The hub features a video, an explainer, a version of the article written for kids, and an editorial, viewpoints, and policy outlook from other eminent experts: Prof David Almeida (Penn State University, USA), Prof Pietro Ghezzi (University of Urbino Carlo Bo, Italy), and Dr Ioannis P Androulakis (Rutgers, The State University of New Jersey, USA).
Journal
Frontiers in Science
DOI
10.3389/1239462
Method of Research
Computational simulation/modeling
Subject of Research
Not applicable
Article Title
A multiscale inflammatory map: linking individual stress to societal dysfunction
Article Publication Date
12-Mar-2024
COI Statement
YV is a cofounder of, and stakeholder in, Immunetrics, Inc. and a consultant to Anuna AI. PFMJV is the founder of, and stakeholder in, Eodyne Systems s.l. and Sapiens5 Holding BV. DLK was employed by Tangelo – Intend, Inc. Neither these companies nor the funders mentioned above were involved in the study design, data collection, analysis, interpretation of data, the writing of this article, or the decision to submit it for publication. The companies mentioned above also did not provide funding for the study. The remaining author declares that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest. The authors YV and PV declared that they are editorial board members of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Acadia’s Nuplazid fails PhIII study due to higher-than-expected placebo effect
After years of trying to expand the market territory for Nuplazid, Acadia Pharmaceuticals might have hit a dead end, with a Phase III fail in schizophrenia…
After years of trying to expand the market territory for Nuplazid, Acadia Pharmaceuticals might have hit a dead end, with a Phase III fail in schizophrenia due to the placebo arm performing better than expected.
Steve Davis
“We will continue to analyze these data with our scientific advisors, but we do not intend to conduct any further clinical trials with pimavanserin,” CEO Steve Davis said in a Monday press release. Acadia’s stock $ACAD dropped by 17.41% before the market opened Tuesday.
Pimavanserin, a serotonin inverse agonist and also a 5-HT2A receptor antagonist, is already in the market with the brand name Nuplazid for Parkinson’s disease psychosis. Efforts to expand into other indications such as Alzheimer’s-related psychosis and major depression have been unsuccessful, and previous trials in schizophrenia have yielded mixed data at best. Its February presentation does not list other pimavanserin studies in progress.
The Phase III ADVANCE-2 trial investigated 34 mg pimavanserin versus placebo in 454 patients who have negative symptoms of schizophrenia. The study used the negative symptom assessment-16 (NSA-16) total score as a primary endpoint and followed participants up to week 26. Study participants have control of positive symptoms due to antipsychotic therapies.
The company said that the change from baseline in this measure for the treatment arm was similar between the Phase II ADVANCE-1 study and ADVANCE-2 at -11.6 and -11.8, respectively. However, the placebo was higher in ADVANCE-2 at -11.1, when this was -8.5 in ADVANCE-1. The p-value in ADVANCE-2 was 0.4825.
In July last year, another Phase III schizophrenia trial — by Sumitomo and Otsuka — also reported negative results due to what the company noted as Covid-19 induced placebo effect.
According to Mizuho Securities analysts, ADVANCE-2 data were disappointing considering the company applied what it learned from ADVANCE-1, such as recruiting patients outside the US to alleviate a high placebo effect. The Phase III recruited participants in Argentina and Europe.
Analysts at Cowen added that the placebo effect has been a “notorious headwind” in US-based trials, which appears to “now extend” to ex-US studies. But they also noted ADVANCE-1 reported a “modest effect” from the drug anyway.
Nonetheless, pimavanserin’s safety profile in the late-stage study “was consistent with previous clinical trials,” with the drug having an adverse event rate of 30.4% versus 40.3% with placebo, the company said. Back in 2018, even with the FDA approval for Parkinson’s psychosis, there was an intense spotlight on Nuplazid’s safety profile.
Acadia previously aimed to get Nuplazid approved for Alzheimer’s-related psychosis but had many hurdles. The drug faced an adcomm in June 2022 that voted 9-3 noting that the drug is unlikely to be effective in this setting, culminating in a CRL a few months later.
As for the company’s next R&D milestones, Mizuho analysts said it won’t be anytime soon: There is the Phase III study for ACP-101 in Prader-Willi syndrome with data expected late next year and a Phase II trial for ACP-204 in Alzheimer’s disease psychosis with results anticipated in 2026.
Acadia collected $549.2 million in full-year 2023 revenues for Nuplazid, with $143.9 million in the fourth quarter.
"Beware the Ides of March,” Shakespeare quotes the soothsayer’s warning Julius Caesar about what turned out to be an impending assassination on March 15. The death of American liberty happened around the same time four years ago, when the orders went out from all levels of government to close all indoor and outdoor venues where people gather.
It was not quite a law and it was never voted on by anyone. Seemingly out of nowhere, people who the public had largely ignored, the public health bureaucrats, all united to tell the executives in charge – mayors, governors, and the president – that the only way to deal with a respiratory virus was to scrap freedom and the Bill of Rights.
And they did, not only in the US but all over the world.
The forced closures in the US began on March 6 when the mayor of Austin, Texas, announced the shutdown of the technology and arts festival South by Southwest. Hundreds of thousands of contracts, of attendees and vendors, were instantly scrapped. The mayor said he was acting on the advice of his health experts and they in turn pointed to the CDC, which in turn pointed to the World Health Organization, which in turn pointed to member states and so on.
There was no record of Covid in Austin, Texas, that day but they were sure they were doing their part to stop the spread. It was the first deployment of the “Zero Covid” strategy that became, for a time, official US policy, just as in China.
It was never clear precisely who to blame or who would take responsibility, legal or otherwise.
This Friday evening press conference in Austin was just the beginning. By the next Thursday evening, the lockdown mania reached a full crescendo. Donald Trump went on nationwide television to announce that everything was under control but that he was stopping all travel in and out of US borders, from Europe, the UK, Australia, and New Zealand. American citizens would need to return by Monday or be stuck.
Americans abroad panicked while spending on tickets home and crowded into international airports with waits up to 8 hours standing shoulder to shoulder. It was the first clear sign: there would be no consistency in the deployment of these edicts.
There is no historical record of any American president ever issuing global travel restrictions like this without a declaration of war. Until then, and since the age of travel began, every American had taken it for granted that he could buy a ticket and board a plane. That was no longer possible. Very quickly it became even difficult to travel state to state, as most states eventually implemented a two-week quarantine rule.
The next day, Friday March 13, Broadway closed and New York City began to empty out as any residents who could went to summer homes or out of state.
On that day, the Trump administration declared the national emergency by invoking the Stafford Act which triggers new powers and resources to the Federal Emergency Management Administration.
In addition, the Department of Health and Human Services issued a classified document, only to be released to the public months later. The document initiated the lockdowns. It still does not exist on any government website.
The White House Coronavirus Response Task Force, led by the Vice President, will coordinate a whole-of-government approach, including governors, state and local officials, and members of Congress, to develop the best options for the safety, well-being, and health of the American people. HHS is the LFA [Lead Federal Agency] for coordinating the federal response to COVID-19.
Closures were guaranteed:
Recommend significantly limiting public gatherings and cancellation of almost all sporting events, performances, and public and private meetings that cannot be convened by phone. Consider school closures. Issue widespread ‘stay at home’ directives for public and private organizations, with nearly 100% telework for some, although critical public services and infrastructure may need to retain skeleton crews. Law enforcement could shift to focus more on crime prevention, as routine monitoring of storefronts could be important.
In this vision of turnkey totalitarian control of society, the vaccine was pre-approved: “Partner with pharmaceutical industry to produce anti-virals and vaccine.”
The National Security Council was put in charge of policy making. The CDC was just the marketing operation. That’s why it felt like martial law. Without using those words, that’s what was being declared. It even urged information management, with censorship strongly implied.
The timing here is fascinating. This document came out on a Friday. But according to every autobiographical account – from Mike Pence and Scott Gottlieb to Deborah Birx and Jared Kushner – the gathered team did not meet with Trump himself until the weekend of the 14th and 15th, Saturday and Sunday.
According to their account, this was his first real encounter with the urge that he lock down the whole country. He reluctantly agreed to 15 days to flatten the curve. He announced this on Monday the 16th with the famous line: “All public and private venues where people gather should be closed.”
This makes no sense. The decision had already been made and all enabling documents were already in circulation.
There are only two possibilities.
One: the Department of Homeland Security issued this March 13 HHS document without Trump’s knowledge or authority. That seems unlikely.
Two: Kushner, Birx, Pence, and Gottlieb are lying. They decided on a story and they are sticking to it.
Trump himself has never explained the timeline or precisely when he decided to greenlight the lockdowns. To this day, he avoids the issue beyond his constant claim that he doesn’t get enough credit for his handling of the pandemic.
With Nixon, the famous question was always what did he know and when did he know it? When it comes to Trump and insofar as concerns Covid lockdowns – unlike the fake allegations of collusion with Russia – we have no investigations. To this day, no one in the corporate media seems even slightly interested in why, how, or when human rights got abolished by bureaucratic edict.
As part of the lockdowns, the Cybersecurity and Infrastructure Security Agency, which was and is part of the Department of Homeland Security, as set up in 2018, broke the entire American labor force into essential and nonessential.
They also set up and enforced censorship protocols, which is why it seemed like so few objected. In addition, CISA was tasked with overseeing mail-in ballots.
Only 8 days into the 15, Trump announced that he wanted to open the country by Easter, which was on April 12. His announcement on March 24 was treated as outrageous and irresponsible by the national press but keep in mind: Easter would already take us beyond the initial two-week lockdown. What seemed to be an opening was an extension of closing.
This announcement by Trump encouraged Birx and Fauci to ask for an additional 30 days of lockdown, which Trump granted. Even on April 23, Trump told Georgia and Florida, which had made noises about reopening, that “It’s too soon.” He publicly fought with the governor of Georgia, who was first to open his state.
Before the 15 days was over, Congress passed and the president signed the 880-page CARES Act, which authorized the distribution of $2 trillion to states, businesses, and individuals, thus guaranteeing that lockdowns would continue for the duration.
There was never a stated exit plan beyond Birx’s public statements that she wanted zero cases of Covid in the country. That was never going to happen. It is very likely that the virus had already been circulating in the US and Canada from October 2019. A famous seroprevalence study by Jay Bhattacharya came out in May 2020 discerning that infections and immunity were already widespread in the California county they examined.
What that implied was two crucial points: there was zero hope for the Zero Covid mission and this pandemic would end as they all did, through endemicity via exposure, not from a vaccine as such. That was certainly not the message that was being broadcast from Washington. The growing sense at the time was that we all had to sit tight and just wait for the inoculation on which pharmaceutical companies were working.
By summer 2020, you recall what happened. A restless generation of kids fed up with this stay-at-home nonsense seized on the opportunity to protest racial injustice in the killing of George Floyd. Public health officials approved of these gatherings – unlike protests against lockdowns – on grounds that racism was a virus even more serious than Covid. Some of these protests got out of hand and became violent and destructive.
Meanwhile, substance abuse rage – the liquor and weed stores never closed – and immune systems were being degraded by lack of normal exposure, exactly as the Bakersfield doctors had predicted. Millions of small businesses had closed. The learning losses from school closures were mounting, as it turned out that Zoom school was near worthless.
It was about this time that Trump seemed to figure out – thanks to the wise council of Dr. Scott Atlas – that he had been played and started urging states to reopen. But it was strange: he seemed to be less in the position of being a president in charge and more of a public pundit, Tweeting out his wishes until his account was banned. He was unable to put the worms back in the can that he had approved opening.
By that time, and by all accounts, Trump was convinced that the whole effort was a mistake, that he had been trolled into wrecking the country he promised to make great. It was too late. Mail-in ballots had been widely approved, the country was in shambles, the media and public health bureaucrats were ruling the airwaves, and his final months of the campaign failed even to come to grips with the reality on the ground.
At the time, many people had predicted that once Biden took office and the vaccine was released, Covid would be declared to have been beaten. But that didn’t happen and mainly for one reason: resistance to the vaccine was more intense than anyone had predicted. The Biden administration attempted to impose mandates on the entire US workforce. Thanks to a Supreme Court ruling, that effort was thwarted but not before HR departments around the country had already implemented them.
As the months rolled on – and four major cities closed all public accommodations to the unvaccinated, who were being demonized for prolonging the pandemic – it became clear that the vaccine could not and would not stop infection or transmission, which means that this shot could not be classified as a public health benefit. Even as a private benefit, the evidence was mixed. Any protection it provided was short-lived and reports of vaccine injury began to mount. Even now, we cannot gain full clarity on the scale of the problem because essential data and documentation remains classified.
After four years, we find ourselves in a strange position. We still do not know precisely what unfolded in mid-March 2020: who made what decisions, when, and why. There has been no serious attempt at any high level to provide a clear accounting much less assign blame.
Not even Tucker Carlson, who reportedly played a crucial role in getting Trump to panic over the virus, will tell us the source of his own information or what his source told him. There have been a series of valuable hearings in the House and Senate but they have received little to no press attention, and none have focus on the lockdown orders themselves.
The prevailing attitude in public life is just to forget the whole thing. And yet we live now in a country very different from the one we inhabited five years ago. Our media is captured. Social media is widely censored in violation of the First Amendment, a problem being taken up by the Supreme Court this month with no certainty of the outcome. The administrative state that seized control has not given up power. Crime has been normalized. Art and music institutions are on the rocks. Public trust in all official institutions is at rock bottom. We don’t even know if we can trust the elections anymore.
In the early days of lockdown, Henry Kissinger warned that if the mitigation plan does not go well, the world will find itself set “on fire.” He died in 2023. Meanwhile, the world is indeed on fire. The essential struggle in every country on earth today concerns the battle between the authority and power of permanent administration apparatus of the state – the very one that took total control in lockdowns – and the enlightenment ideal of a government that is responsible to the will of the people and the moral demand for freedom and rights.
How this struggle turns out is the essential story of our times.
CODA: I’m embedding a copy of PanCAP Adapted, as annotated by Debbie Lerman. You might need to download the whole thing to see the annotations. If you can help with research, please do.
We use cookies on our website to give you the most relevant experience by remembering your preferences and repeat visits. By clicking “Accept”, you consent to the use of ALL the cookies.
This website uses cookies to improve your experience while you navigate through the website. Out of these, the cookies that are categorized as necessary are stored on your browser as they are essential for the working of basic functionalities of the website. We also use third-party cookies that help us analyze and understand how you use this website. These cookies will be stored in your browser only with your consent. You also have the option to opt-out of these cookies. But opting out of some of these cookies may affect your browsing experience.
Necessary cookies are absolutely essential for the website to function properly. These cookies ensure basic functionalities and security features of the website, anonymously.
Cookie
Duration
Description
cookielawinfo-checbox-analytics
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Analytics".
cookielawinfo-checbox-functional
11 months
The cookie is set by GDPR cookie consent to record the user consent for the cookies in the category "Functional".
cookielawinfo-checbox-others
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Other.
cookielawinfo-checkbox-necessary
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookies is used to store the user consent for the cookies in the category "Necessary".
cookielawinfo-checkbox-performance
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Performance".
viewed_cookie_policy
11 months
The cookie is set by the GDPR Cookie Consent plugin and is used to store whether or not user has consented to the use of cookies. It does not store any personal data.
Functional cookies help to perform certain functionalities like sharing the content of the website on social media platforms, collect feedbacks, and other third-party features.
Performance cookies are used to understand and analyze the key performance indexes of the website which helps in delivering a better user experience for the visitors.
Analytical cookies are used to understand how visitors interact with the website. These cookies help provide information on metrics the number of visitors, bounce rate, traffic source, etc.
Advertisement cookies are used to provide visitors with relevant ads and marketing campaigns. These cookies track visitors across websites and collect information to provide customized ads.














































{kind=link}