Philippines, Brazil Interested In Russian COVID-19 Vaccine; Australia Suffers Deadliest Day Yet: Live UpdatesTyler DurdenWed, 08/12/2020 - 07:56
Summary:
Brazil, Philippines review Russian vaccine
Australia suffers deadliest day yet; first day north of 400 new cases in 3
Duterte says he would personally take Russian vaccine
Tokyo confirms 222 new cases
South Korea tightens some restrictions amid mild uptick
German health minister "skeptical" of Russian vaccine
* * *
Russian authorities are engaging with the WHO about the possibility of "preapproving" Russia's first COVID-19 vaccine, which has only been tested on a few hundreds people. However, while western governments and officials like Dr. Scott Gottlieb express skepticism, other countries suffering from untrammeled outbreaks are trying to find ways to engage.
Responding to these criticisms, Russia's Health Minister Mikhail Murashko said allegations that Russia's COVID-19 vaccine is unsafe are "groundless" and "driven by competition."
Local press reports that Brazil's Parana state is in talks to produce a Russia-approved COVID-19 vaccine, despite not having completed mass clinical trials. However, it's unclear whether Brazil's regulators would grant this approval.
During yesterday's Moscow conference dedicated to introducing the adenovirus-vaccine to the world, the CEO of the Russian Direct Investment Fund explained that it had already received orders for a billion doses.
"Together with our foreign partners, we are ready to produce more than 500 million doses of the vaccine per year," fund CEO Kirill Dmitriev explained. Everything produced in Russia will be used domestically, and doses produced abroad will be consumed abroad, he said.
Already on Wednesday, Philippine scientists were set to meet representatives of the Gameleya Research Institute, which spear-headed testing of the vaccine with Moscow's state medical college. Philippine President Rodrigo Duterte has already congratulated Russia on its vaccine, and offered to be "injected in public" to allay fears surrounding safety.
Meanwhile, German Health Minister Jens Spahn said during a radio interview that he’s “very skeptical” about Russia's COVID-19 vaccine, which is cleared for use but could be dangerous to use."
"It’s not about being first, it’s about having an effective, tested and therefore safe vaccine," said Spahn on DLF radio.
British newspaper the Telegraph warned in an editorial published with Wednesday's edition that the world should be skeptical of Russia's vaccine since it has only undergone limited testing for safety and efficacy. Despite the Gameleya Institute's solid track record for producing vaccines, a legacy that Putin leaned on heavily during Tuesday's press briefing, the editorial warned to be wary of "political" ploys.
The epidemiology it is using is similar to that at Oxford University where scientists are also said to be close to success. But the requisite protocols for determining whether the Russian vaccine is both safe and effective do not yet appear to have been carried out. The numbers involved in clinical trials are also low which makes efficacy hard to establish.
Furthermore, the fact that the Russians have called the vaccine Sputnik 5 after the Soviet satellite that stole a march on the Americans in the Sixties by sending animals into space and returning them to Earth indicates a political agenda.
Tokyo confirmed 222 new coronavirus infections, compared with 188 the previous day and 197 on Monday.
One day after confirming its first domestic cases in 102 days, New Zealand Prime Minister Jacinda Ardern said her cabinet would decide Friday on "next steps" re: any new COVID-19 restrictions.
South Korea, meanwhile, confirmed 54 new cases, up from 34 a day ago, pushing total infections in the country to 14,714 with 305 deaths. In response, the government strengthened social distancing rules in funeral homes and wedding halls to prevent the contagion's spread.
Finally, one week after Melbourne extended a temporary lockdown in response to the outbreak in Victoria, Australia recorded its deadliest day of the pandemic on Wednesday, and the biggest daily rise in infections in three days, denting hopes that a second wave gripping the state of Victoria may be stabilizing. Victoria reported 21 deaths, two more than the previous deadliest day earlier this week. The country reported also reported 410 new cases in the past 24 hours, snapping a stretch of 3 days with fewer than 400 cases.
Glimpse Of Sanity: Dartmouth Returns Standardized Testing For Admission After Failed Experiment
In response to the virus pandemic and nationwide Black Lives Matter riots in the summer of 2020, some elite colleges and universities shredded testing requirements for admission. Several years later, the test-optional admission has yet to produce the promising results for racial and class-based equity that many woke academic institutions wished.
The failure of test-optional admission policies has forced Dartmouth College to reinstate standardized test scores for admission starting next year. This should never have been eliminated, as merit will always prevail.
"Nearly four years later, having studied the role of testing in our admissions process as well as its value as a predictor of student success at Dartmouth, we are removing the extended pause and reactivating the standardized testing requirement for undergraduate admission, effective with the Class of 2029," Dartmouth wrote in a press release Monday morning.
"For Dartmouth, the evidence supporting our reactivation of a required testing policy is clear. Our bottom line is simple: we believe a standardized testing requirement will improve—not detract from—our ability to bring the most promising and diverse students to our campus," the elite college said.
Who would've thought eliminating standardized tests for admission because a fringe minority said they were instruments of racism and a biased system was ever a good idea?
Also, it doesn't take a rocket scientist to figure this out. More from Dartmouth, who commissioned the research:
They also found that test scores represent an especially valuable tool to identify high-achieving applicants from low and middle-income backgrounds; who are first-generation college-bound; as well as students from urban and rural backgrounds.
All the colleges and universities that quickly adopted test-optional admissions in 2020 experienced a surge in applications. Perhaps the push for test-optional was under the guise of woke equality but was nothing more than protecting the bottom line for these institutions.
A glimpse of sanity returns to woke schools: Admit qualified kids. Next up is corporate America and all tiers of the US government.
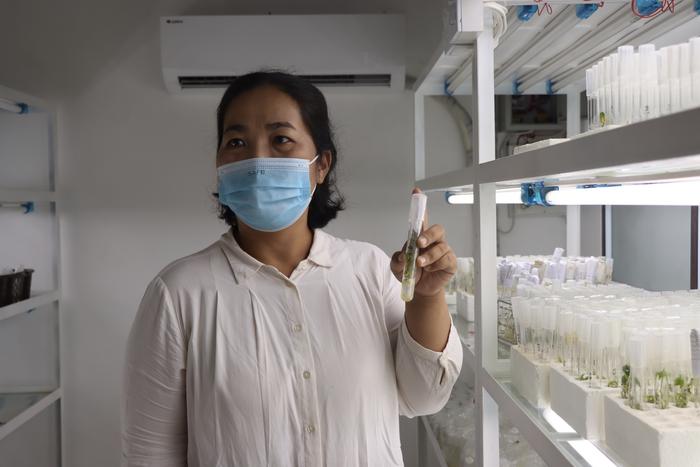
In a recent breakthrough, DNA sequencing technology has uncovered the culprit behind cassava witches’ broom disease: the fungus genus Ceratobasidium.
Credit: Alliance of Bioversity and CIAT / A. Galeon
In a recent breakthrough, DNA sequencing technology has uncovered the culprit behind cassava witches’ broom disease: the fungus genus Ceratobasidium.
The cutting-edge nanopore technology used for this discovery was first developed to track the COVID-19 virus in Colombia, but is equally suited to identifying and reducing the spread of plant viruses. The findings, published in Scientific Reports, will help plant pathologists in Laos, Cambodia, Vietnam and Thailand protect farmers’ valued cassava harvest.
“In Southeast Asia, most smallholder farmers rely on cassava: its starch-rich roots form the basis of an industry that supports millions of producers. In the past decade, however, Cassava Witches’ Broom disease has stunted plants, reducing harvests to levels that barely permit affected farmers to make a living,” said Wilmer Cuellar, Senior Scientist at the Alliance of Bioversity and CIAT.
Since 2017, researchers at the Alliance of Bioversity International and CIAT have incorporated nanotechnology into their research, specifically through the Oxford Nanopore DNA/RNA sequencing technology. This advanced tool provides insight into the deeper mysteries of plant life, accurately identifying pathogens such as viruses, bacteria and fungi that affect crops.
“When you find out which pathogen is present in a crop, you can implement an appropriate diagnostic method, search for resistant varieties and integrate that diagnosis into variety selection processes,” said Ana Maria Leiva, Senior Researcher at the Alliance.
Nanotechnology, in essence, is the bridge between what we see and what we can barely imagine. This innovation opens a window into the microscopic world of plant life and pathogens, redefining the way we understand and combat diseases that affect crops.
For an in-depth look at the technology being used in Laos and Colombia, please explore this link.
About the Alliance of Bioversity International and CIAT
The Alliance of Bioversity International and the International Center for Tropical Agriculture (CIAT) delivers research-based solutions that harness agricultural biodiversity and sustainably transform food systems to improve people’s lives. Alliance solutions address the global crises of malnutrition, climate change, biodiversity loss, and environmental degradation.
With novel partnerships, the Alliance generates evidence and mainstreams innovations to transform food systems and landscapes so that they sustain the planet, drive prosperity, and nourish people in a climate crisis.
The Alliance is part of CGIAR, a global research partnership for a food-secure future. www.alliancebioversityciat.org
Journal
Scientific Reports
DOI
10.1038/s41598-023-49735-5
Method of Research
Content analysis
Subject of Research
Cells
Article Title
Ceratobasidium sp. is associated with cassava witches’ broom disease, a re-emerging threat to cassava cultivation in Southeast Asia
There are many ways to privately improve public health. Such responses make use of local knowledge, entrepreneurship, and civil society and pursue standard…
There are many ways to privately improve public health. Such responses make use of local knowledge, entrepreneurship, and civil society and pursue standard goals of public health like controlling the spread of infectious diseases. Moreover, private responses improve overall welfare by lowering the total costs of a disease and limiting externalities. If private responses can produce similar outcomes as standard, governmental public health programs—and more—perhaps we should reconsider when and where we call upon governments to improve public health.
Two Kinds of Private Responses
Following Vernon Smith and his distinction between constructivist and ecological rationality, private actors can engage in two general kinds of public health improvements. They can engage in concerted efforts to improve public health, and they can engage in emergent responses through myriad interactions.1 Three stories below—about William Walsh, Martha Claghorn, and Edwin Gould—indicate concerted efforts to improve public health.
Walsh, a Catholic priest and President of the Father Matthew Society in Memphis, Tennessee, used the society to organize a refugee camp outside of the city and helped hundreds of people avoid yellow fever during the 1878 epidemic—one of the worst yellow fever epidemics in the country.2 Shortly after learning mosquitos carried diseases prior to 1901, Claghorn chaired the Civics committee of the Twentieth Century Club in the Richmond Hill area of Long Island and led a community-wide anti-mosquito campaign, which rid the area of potentially infectious mosquitos.3 After realizing that many of his employees were sick with malaria, Gould—president of the St. Louis Southwestern Railway—used his wealth and business firm to finance and develop an anti-mosquito campaign throughout Texas.4
These stories show how individuals recognize a public health problem given their circumstances and use their knowledge and available resources to resolve the problem. More recently, we might all be familiar with private, constructivist responses to Covid-19. We all made plans to avoid others and produce our desired amount of exposure. Many people made facemasks from old clothes or purchased them from facemask producers. Businesses, retailers, restaurants, and many others adapted in various ways to limit exposure for their workers and customers. My favorite example, albeit not relevant for most, is the so-called bubble that was implemented by the NBA, which housed teams, encouraged play, and limited infection. The NBA finished their season and crowned a 2020 champion only because of the privately designed and implemented bubble solution. The key is that the bubble pursued all of those objectives, not just one of them. All of these responses indicate how private interactions among people can minimize their exposure, through negotiation, discussion, and mutually beneficial means.
In addition to privately designed solutions, emergent public health responses are also important, perhaps even more so. Long-term migration and settlement patterns away from infectious diseases, consumption to improve nutrition, hygiene, sanitation, and the development of social norms to encourage preventative behavior are all different kinds of emergent public health responses. Each of these responses—developed through the actions of no one person—are substantial ways to improve public health.
First, consider how common migration operates as a means of lowering prevalence rates. As soon as people realized that living near stagnant bodies of water increased the probability of acquiring diseases like malaria, they were more likely to leave those areas and subsequently avoid them. Places with such features became known as places to avoid; people also developed myths to dissuade visitors and inhabitants.5 Such myths and associations left places like the Roman Campagna desolate for centuries. These kinds of cultural associations are also widespread; for example, many people in North and South Carolina moved to areas with higher elevation and took summer vacations to avoid diseases like malaria. East End and West End, in London, also developed because of the opportunities people had to migrate away from (and towards) several diseases.6
While these migration patterns might develop over decades, movement and migration also help in more acute public health crises. During the 1878 yellow fever epidemic throughout the southern United States, for example, thousands of people fled their cities to avoid infection. They took any means of transportation they could find. While some fled to other, more northern cities, many acquired temporary housing in suburbs, and many formed campsites and refugee camps outside of their city. The refugee camps outside of Memphis—like the one formed by William Walsh—helped hundreds and thousands of people avoid infection throughout the Fall of 1878.
Second, more mundane public health improvements—like improvements in nutrition, hygiene, and sanitation—are also emergent. These improvements arise from the actions of individuals and entrepreneurs, often closely associated with voluntary consumption and markets. According to renowned medical scientist Thomas McKeown, that is, rising incomes encouraged voluntary changes in consumption, which helped improve nutrition, sanitation, and lowered mortality rates.7 These effects were especially pertinent for women and mothers as they often selected more nutritious food and altered household sanitation practices. With advancing ideas about germs, moreover, historian Nancy Tomes argues that private interests advanced the campaign to improve house-hold sanitation and nutrition—full of advice and advertisements in newspapers, magazines, manuals, and books.8 Following Tomes, economic historians Rebecca Stein and Joel Mokyr substantiate these ideas and show that people changed their hygiene, sanitation, house-hold cleaning habits, and diets as they learned more about germs.9 Such developments helped people to provide their desired exposure to germs according to their values.
Obviously, there were concerted public health improvements during this time that also explain falling mortality rates. For example, waterworks were conscious efforts to improve public health and were provided publicly and privately, with similar, positive effects on health.10 The point is that while we might be quick to connect the health improvements associated with a public water system, we should also recognize emergent responses like gradual changes in voluntary consumption.
Finally, social norms or rules that encourage preventative behavior might also be relevant kinds of emergent public health responses. Such rules identify behavior that should or should not be allowed, they are enforced in a decentralized way, and if they follow from the values of individuals in a community.11 If such rules pertain to public health, they can raise the cost of infectious behavior or the benefits of preventative behavior. Covering one’s mouth when sneezing is not only beneficial from a public health perspective, it also helps avoid earning disapproval.
The condom code during the height of the HIV/AIDS epidemic is another example of an emergent public health rule that reduced infectiousness by encouraging safer behavior.12 People who adopted safer sexual practices were seen to be doing the right thing—akin to taking care of a brother. People who refrained from adopting safer sexual practices were admonished. No single person or entity announced the rule; rather, it emerged from the actions and interactions of individuals within various communities to pursue their goals regarding maintaining sexual activity and limiting the spread of disease. Indeed, such norms were more effective in communities where people used their social capital resources to determine which behaviors should be changed and where they can more easily monitor and enforce infractions. This seems like a relevant factor where many gay men and men who have sex with men live in dense urban areas like New York and Los Angeles that foster LGBTQ communities.
Covid-19 provides additional examples where social norms encouraged the use of seemingly appropriate behavior, e.g., social distancing, the use of facemasks, and vaccination. Regardless of any formal rule in place, many people adapted their behavior because of social norms that encouraged social distancing, the use of facemasks, and vaccination. In communities that valued such behaviors, people that wore face masks and vaccinated were praised and were seen as doing the right thing; people that did not were viewed with scorn. Indeed, states and cities that have higher levels of social capital and higher values for public health tend to have higher Covid-19 vaccine uptakes.13
Improving Public Health and More
“Private approaches tend to lower the total costs of diseases and they limit externalities.”
While these private approaches can improve public health, can they do more than typical public health approaches cannot? Private approaches tend to lower the total costs of diseases and they limit externalities. Each aspect of private responses requires additional explanation.
Responding to infectious diseases and disease prevention is doubly challenging because not only do we have to worry about being sick, we also have to consider the costs imposed by our preventative behaviors and the rules we might impose. Thus, the total costs of an infectious disease include 1) the costs related to the disease—the pain and suffering of a disease and the opportunity costs of being sick—and 2) the costs associated with preventative and avoidance behavior. While disease costs are mostly self-explanatory, the costs of avoiding infection warrant more explanation. Self-isolation when you have a cold, for example, entails the loss of potentially valuable social activities; and wearing condoms to prevent sexually transmitted diseases forfeits the pleasures of unprotected sexual activity. Diseases for which vaccines and other medicines are available are less worrisome, perhaps, because these are diseases with lower prevention costs than diseases where those pharmaceutical interventions are not available. Governmental means of prevention also add relevant costs. Many readers might be familiar with the costs imposed by our private and public responses to Covid—from isolation to learning loss, and from sharp decreases in economic activity to increased rates of depression and spousal abuse.14 Long before Covid, moreover, people bemoaned wearing masks during the Great Flu,15 balked at quarantine against yellow fever,16 and protested bathhouse closings with the onset of HIV.17
Figure 1 shows the overall problem: diseases are harmful but our responses to those diseases might also be harmful.
Figure 1. The Excess Burden of Infectious Diseases
This figure follows Bhattacharya, Hyde, and Tu (2013) and Philipson (2000), who refer to the difference between total costs and disease costs as the excess burden of a disease. That is, excess burden depends on how severely we respond to a disease in private and in public. The excess burden associated with the common cold tends to be negligible as we bear the minor inconvenience of a fever, a sore throat perhaps, or a couple days off work; moreover, most people don’t go out of their way to avoid catching a cold. The excess burden of plague, however, is more complicated; not only are the symptoms much worse—and include death—people have more severe reactions. Note too that disease costs rise with prevalence and with worsening symptoms but eventually decline as more severe diseases tend to be less prevalent. Still, no one wants to be infected with a major disease, and severe precautions are likely. We might shun all social interactions, and we might use government to impose strict quarantine measures. As disease severity rises along the horizontal axis, it might be the case that the cure is worse than the disease.
The private responses indicated above all help to lower the total costs of a disease because people choose their responses and they use their local knowledge and available resources to select cheaper methods of prevention. Claghorn used her neighborhood connections and the social capital of her civics association to encourage homeowners to rid their yards of pools of water; as such she lowered the costs of producing mosquito control. Similarly, Gould used the organizational structure of his firm to hire experts in mosquito control and build a sanitation department. These are cheap methods to limit exposure to mosquitos.
Emergent responses also help to lower the total costs of a disease because such responses indicate the variety of choices people face and their ability to select cheaper options. People facing diseases like malaria might be able to move away and, for some, it is cheaper than alternative means of prevention. Many people now are able to limit their exposure to mosquitos with screens, improved dwellings, and air conditioning.18 Consider the variety of ways people can limit their exposure to sexually transmitted diseases like HIV. If some people would rather use condoms to limit HIV transmission, they are better off doing so than if they were to refrain from sexual activity altogether. Similarly, some people would be better off having relatively risky sexual activity if they were in monogamous relationships or if they knew about their partner’s sexual history. That people can choose their own preventative measures indicates lower total costs compared with blunt, one-rule-for-all, governmental public health responses.
Negative and positive externalities of spreadable diseases indicate too much infectious behavior and too little preventative behavior, respectively. Hosting a party is fun, but it also incurs the internal costs of the drinks and appetizers and, more importantly, perhaps the external costs of raising the probability that people get sick. Attending a local cafe can be relaxing, but you have to pay for a cup of coffee and you might also transmit a disease to other coffee drinkers. The same could be said for many other public and social activities that might spread diseases like attending a class or a basketball game, transporting goods and people, and sexual behaviors. Our preventative behaviors from taking a vaccine to covering your mouth and from isolation to engaging in safer sexual practices emits positive externalities. If left unchecked, negative and positive externalities lead to higher rates of infection.
Overall, we should continue to think more critically about delineating how private and public actors can improve public health and overall welfare. More importantly, we should recognize that private actors are more capable than we often realize, especially in light of conscious efforts to improve public health and those efforts that emerge from people’s actions and interactions. These private efforts might be better at advancing some public health goals than public actors do. Individuals, for example, have more access to local knowledge and can discover novel solutions that serve multiple ends—often ends they value—rather than the ends of distant officials. Such cases and possibilities indicate cheaper ways to improve public health.
Footnotes
[1] Smith (2009), Rationality in Economics: Constructivist and Ecological Forms, Cambridge University Press.
[2] For more on Walsh, see Carson (forthcoming), “Prevention Externalities: Private and Public Responses to the 1878 Yellow Fever Epidemic,” Public Choice.
[3] For more on Claghorn, see Carson (2020), “Privately Preventing Malaria in the United States, 1900-1925,” Essays in Economics and Business History.
[4] For more on Gould, see Carson (2016), “Firm-led Malaria Prevention in the United States, 1910-1920,” American Journal of Law and Medicine.
[5] On the connection between malarial diseases, dragons, and dragon-slaying saints, see Horden (1992), “Disease, Dragons, and Saints: the management of epidemics in the dark ages,” in Epidemics and Ideas by Ranger and Slack.
[6] For more on migration and prevalence rates, see Mesnard and Seabright (2016), “Migration and the equilibrium prevalence of infectious disease,” Journal of Demographic Economics.
[8] Tomes (1990), “The Private Side of Public Health: Sanitary Science, Domestic Hygiene, and the Germ Theory, 1870-1990,” Bulletin of the History of Medicine.
[9] Mokyr and Stein (1996), “Science, Health, and Household Technology: The Effect of the Pasteur Revolution on Consumer Demand,” in The Economics of New Goods, NBER.
[10] See Werner Troesken’s work on public and private waterworks in the U.S. around the turn of the 20th century. See Galiani, Gertler, and Shargrodsky (2005), “Water for Life,” Journal of Political Economy.
[11] Brennan et al., (2013), Explaining Norms, Oxford University Press.
[12] For more on the condom code, see Carson (2017), “The Informal Norms of HIV Prevention: The emergence and erosion of the condom code,” Journal of Law, Medicine and Ethics.
[13] Carilli, Carson, and Isaacs (2022), “Jabbing Together? The complementarity between social capital, formal public health rules, and covid-19 vaccine rates in the U.S.,” Vaccine.
[14] Leslie and Wilson, “Sheltering in Place and Domestic Violence: Evidence from Calls for Service During Covid-19.” Journal of Public Economics 189, 104241. Mulligan, “Deaths of Despair and the Incidence of Excess Mortality in 2020,” NBER, https://www.nber.org/papers/w28303. Betthauser, Bach-Mortensen, and Engzell, “A systematic review and meta-analysis of the evidence on learning during the Covid-19 Pandemic,” Nature Human Behavior, https://www.nature.com/articles/s41562-022-01506-4
[18] Tusting et al. (2017), “Housing Improvement and Malaria Risk in Sub-Saharan Africa: a multi-country analysis of survey data.” PLOS Medicine.
*Byron Carson is an Associate Professor of Economics and Business at Hampden-Sydney College in Virginia, where he teaches courses on introductory economics, money and banking, health economics, and urban economics. Byron earned his Ph.D. in Economics from George Mason University in 2017, and his research interests include economic epidemiology, public choice, and Austrian economics.
This article was edited by Features Editor Ed Lopez.
We use cookies on our website to give you the most relevant experience by remembering your preferences and repeat visits. By clicking “Accept”, you consent to the use of ALL the cookies.
This website uses cookies to improve your experience while you navigate through the website. Out of these, the cookies that are categorized as necessary are stored on your browser as they are essential for the working of basic functionalities of the website. We also use third-party cookies that help us analyze and understand how you use this website. These cookies will be stored in your browser only with your consent. You also have the option to opt-out of these cookies. But opting out of some of these cookies may affect your browsing experience.
Necessary cookies are absolutely essential for the website to function properly. These cookies ensure basic functionalities and security features of the website, anonymously.
Cookie
Duration
Description
cookielawinfo-checbox-analytics
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Analytics".
cookielawinfo-checbox-functional
11 months
The cookie is set by GDPR cookie consent to record the user consent for the cookies in the category "Functional".
cookielawinfo-checbox-others
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Other.
cookielawinfo-checkbox-necessary
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookies is used to store the user consent for the cookies in the category "Necessary".
cookielawinfo-checkbox-performance
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Performance".
viewed_cookie_policy
11 months
The cookie is set by the GDPR Cookie Consent plugin and is used to store whether or not user has consented to the use of cookies. It does not store any personal data.
Functional cookies help to perform certain functionalities like sharing the content of the website on social media platforms, collect feedbacks, and other third-party features.
Performance cookies are used to understand and analyze the key performance indexes of the website which helps in delivering a better user experience for the visitors.
Analytical cookies are used to understand how visitors interact with the website. These cookies help provide information on metrics the number of visitors, bounce rate, traffic source, etc.
Advertisement cookies are used to provide visitors with relevant ads and marketing campaigns. These cookies track visitors across websites and collect information to provide customized ads.





























{kind=link}