I mean, who wants to say “living with COVID” amirite? The connotation is that it’s just a necessary thing we have to do. But really, at some point, it kind Read More …
The post Living next door to Alice appeared first on Virology Down Under.
I mean, who wants to say “living with COVID” amirite? The connotation is that it’s just a necessary thing we have to do. But really, at some point, it kind of is necessary just because most of the world hasn’t made good choices to this point and the virus is so widespread that it would take a massive collaborative effort using better vaccines, to ever eliminate COVID-19. Personally, I don’t think it’s realistic to suggest we’re not, let’s say, “living next door to Alice” (here Alice is the virus, SARS-CoV-2, not the disease, COVID-19), for at least years to come.
That’s all a bit hopeless isn’t it?
I don’t think so. Let’s use Australia as a case study because it did so well for so long.
A recent 12-24 period recorded 35,000 positives in Australia. To eliminate the virus from Australia now is almost impossible without:
return of border controls
return of lockdowns
return of masks
return of density caps
return of contact tracing (currently out of control) to capture all cases and contacts
need for PCR – not rapid antigen tests – to catch every positive person and their contacts as early as posisble
return of all quarantine and isolation of cases and contacts
Essentially reinstating every tool we were previously using to allow us to rid the country of every infected person. After which, we’d have to instigate a surveillance system to test every incoming/returning traveller with a possible case of COVID-19 (a lot harder to pick clinically than measles is for example) for SARS-CoV-2.
Can I remind you that a big chunk of cases is asymptomatic and that the symptoms of COVID-19 can include…
fever
cough
tiredness
loss of taste or smell
sore throat
headacheaches and pains
diarrhoeaa
rash on skin
discolouration of fingers or toes
red or irritated eyes
difficulty breathing or shortness of breath
loss of speech or mobility,
confusion
chest pain
Easy to pick that case up, right? No, it isn’t. It needs a laboratory test. It has all along except in rare cases of severe disease. That would have to be done before contact with others, and it would need to be repeated 3-5 days later if you were serious about catching an incubating infection. We’re simply not planning to do that.
We’d have to hunt down every case with testing levels at or beyond the level we have now along with a fully compliant population.
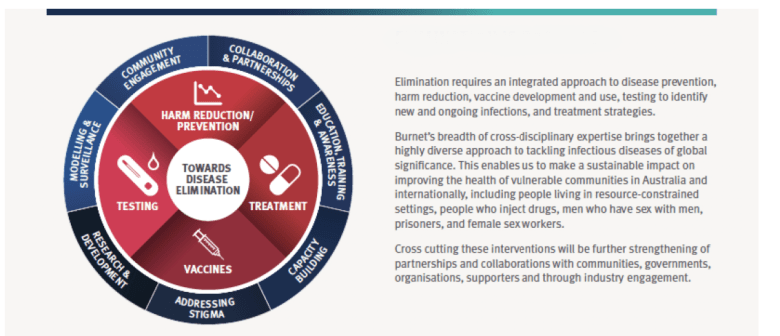
Eliminate virus or disease?
Now the knowledgeable among you will be saying that really, we want to make the country disease-free rather than virus-free. Fair enough. We’ve done that with, for example, measles and rubella in Australia.
Modified from the Burnet Institute.[1]
Vaccines have already gone a very long way towards reducing the levels of severe COVID-19. Not to zero, but then they also don’t do that for other virus-induced diseases.
Biology is a complex beast. There are always people for whom vaccines don’t work or work less effectively. But just as we don’t effectively protect them from death and harm due to influenza, respiratory syncytial virus (RSV) or human metapneumovirus (HMPV) disease, to name a few, we won’t be able to prevent all harm from SARS-CoV-2. Even with better vaccines.
What we can do and have done
We can treat disease better – from steroid treatment to patient placement to new and emerging antiviral sand antibody cocktails – we have quickly increased the arsenal of ways to reduce severe disease.
We can slow transmission – although that isn’t happening in a way that meets expectations almost anywhere (I see you, Kiwiland), even with some mask use. We know that high vaccination levels don’t wholly stop SARS-CoV-2 from spreading.
Immunity from vaccination and infection does reduce the severity of disease because that’s biology and immunology. This virus hasn’t turned it on its head, even if the messaging is confusing and seemingly contradictory.
Keeping in mind that severe disease and death was already at the pointy and rare end of SARS-CoV-2 infections – even though that harm has been tremendous because infections were in such vast numbers. But vaccination has further reduced severe outcomes. Wherever this has been looked at. And with the first booster/3rd dose, this is even more effective at reducing disease after infection.
Perhaps soon, we may stop to think about what we’re expecting to happen with this virus. Are we expecting things to turn out better than we have ever expected with some other far less well quantified viral and bacterial diseases that kill and cause a range of harms (also nowhere near as closely studied as COVID-19’s effects have been)?
Infectious and communicable diseases, Australian Institute of Health and Welfare (AIHW).[2]
It might be time to utter those horrible words again – how does COVID-19 (Omicron in highly vaccinated parts) compare to flu at the moment? It would be nice to have this as a global discussion and not assume this means anyone is downplaying the impact of COVID-19. Perhaps an international health authority could take the lead here; maybe a worldwide simulcast seminar (gasp – think of the educational opportunities)!
But communication is something we aren’t doing well in this latest chapter of the Book of COVID (I think we’ve just written notes on the ‘test wars’ chapter, mainly having completed the ‘vaccine wars’ draft).
Everything is messy right now and the public has not been kept up on what’s happening for a while. We’ve learned nothing about keeping the public informed these past two years, have we?
So what might living next door to Alice look like?
The graphic below got me into trouble on Twitter as it came across as too defeatist for some. The reality is that we haven’t done enough to get rid of the virus, and while the virus exists, there will be asymptomatic, mild and moderate cases of COVID-19.
Australia was in a great place to test what was possible. In the State of Victora, a Wave that reached over 720 cases per day at the end of July 2021 was turned around and driven to zero. At the beginning of September 2021, when Delta started to appear in Victoria again, the will just wasn’t there for another prolonged battle.[3,4,5] The State of New South Wales had already acquiesced to its wave and, after locking down for many weeks, made a conscious decision to discard a COVIDzero approach and more to suppress spread while getting vaccination-induced immunity levels up. That epidemic triggered seeding events all over Australia and into New Zealand.[6] It was apparent then that we had shifted gears and that we couldn’t control this efficient respiratory virus again and again and again. And if we couldn’t handle it at dozens to hundreds of cases, we should honestly embrace the reality that we won’t get to a place where we can control it at thousands and tens of thousands of daily cases, be they local or worldwide. And at some point soon, testing levels will drop as the public realise there is little point in queueing and getting swabbed or paying for rapid antigen tests (RAT) when there are few conditions in place to do anything with those results. Slowly those who are sick “enough” or need evidence that they are infected will get tested. Fever clinics and drive through testing will slow down and pack away. We will know only very approximately how many cases are in the community from at that point. This is a significant shift from the super intense scrutiny of case numbers we’ve had in Australia. Then the media will also stop caring as much. Politicians will have stopped minimising the pandemic and moved on to their pre-election agendas. Sniping at experts, academics and scientists willing to help the public understand what politicians want will fire up – oh sorry, that’s already happening.
Things will return to something like how we dealt with influenza or RSV or MPV. Maybe even in 2022? But the virus will still be there, as will illness and deaths and research reports about all that SARS-COV-2 is capable of.
Even with a great vaccine, there will be those with waning immunity. There will be new birth cohorts with no immunity. There will be those who don’t get vaccinated. There will be those with immune systems that don’t work as well as needed. There will be some with risk factors that may override the protection afforded by vaccine immunity, subjecting them to a baseline of worse outcomes. Together these people will likely see more severe COVID-19. This is a tale that can also be told about other infectious diseases. There is always a proportion we can’t protect. At least, not unless we keep everyone in a bubble or on an IV vaccine or immune stimulant of some sort. Or we collaborate to make the world a better place (but I have no hope of seeing that reality in my time).
We also know that infection and transmission can still happen in the presence of immunity – whether vaccine or infection-induced. Again, this is biology. SARS-CoV-2 will therefore bounce around for a whole range of reasons – some of which I hope I’ve covered above. I may add some in response to the feedback I get to this post. Most of the time, SARS-CoV-2 will be passing along at low levels, constantly evolving, as all the other respiratory viruses do all the time (just because you don’t hear about them or they’re not causing an epidemic, doesn’t mean they’ve disappeared!). Occasionally when habits change, such as when we huddle inside in what will likely remain poorly ventilated spaces for some years yet, to escape the heat or the cold, or when the size of a suitably non-immune population reaches a tipping point, occasional surges or epidemics will result. There could be a role for more dramatic viral changes as well; this virus has infected many animals in the past two years. But it’s my opinion that SARS-CoV-2 will maintain enough transmission to stick with us for many years yet.
It’s just a graphic, not a model.
The below image was an idea I had to try to visualise what life might be like in one version of a future. To be clear, that future could be years away. I put it out on Twitter, and it got refined a little in response to a range of feedback.
It starts with a largely well-vaccinated population with immunity (left-hand side).
Biology and immunology have shown repeatedly that with great immunity (to an infectious thing) comes great protection from the worst of disease (due to infection by most of those things).
In the future, from this mythical future global population (thick central orange line), I’m presuming that the vast majority of infections will be manageable outside of a hospital. That’s not prophetic – because that’s the case now! But even moreso than they are now.
Some infections will not be, and those people will need more care than can be managed at home. Some will, tragically, die. Disproportionately among the unvaccinated. You can see for yourself a pre-Omicron estimate of how age is critical to understanding death (don’t use a single “fatality rate” to describe the impact of SARS-CoV-2).[13]. To be clear, I’m not advocating for any of these deaths, by the way! This is the path that we are all on, though. Like it or argue against it – we’ve done nothing but create and sometimes refine or improve this path.
The graphic also shows the emergence of new variants – when I made it, there was no Omicron. Its appearance proved to be a great example of the puff of purple virions in that bottom loop.
I expect childhood vaccination programs to reduce an already low likelihood of severe disease in the young. Such programs will create an immune population that will travel with that immunity. Don’t forget SARS-CoV (the original). Cases still have cellular immune memory a dozen years later, which probably protects from severe disease (because that’s how it usually works). SARS-CoV-2 vaccines also generate such immunity, even across the variant spectrum.[10]. Immunity will dampen severity.
Life (right-hand side) will contain additional shots and better vaccines or boosters to prevent disease and new drugs to treat the condition. Ongoing reinfections will happen – as they do for other viruses – but these will mostly be non-severe diseases or be asymptomatic.
Future variants – the bottom loop – are not guaranteed to be milder than previous ones. They just need to have some advantage that allows them to keep passing from one cell sack (host) to another. Whatever mutations accompany a change to a virus that makes that viral variant better in a significant way will stick. If other mutations co-occur that cause us to slowly melt or bleed from the eyes, that’s what would & could happen. But immunity has reached levels that it’s never been at before, so it will look like new variants arent; as bad for all but the more nasty, virulent newly emerged immune escape variants. Don’t fall for that “Ohhh, but it wouldn’t be advantageous to the virus” unimaginative rubbish. If a virus passes on its genes before its host dies, then mission accomplished in virus land. You could still bleed from the eyes & pass on a virus. You could still melt much later & still pass it on.
To reiterate – immunity developed after a symptomatic infection dramatically reduces the risk of future severe disease from reinfection. That immune memory lingers in most of usfor life in some form at some level of effectiveness.
But Living Next Door to Alice is still confounded by one big unknown.
The exhausted elephant in the room
Many people infected by SARS-CoV-2 recover without problems. However, some proportion is left with persistent symptoms commonly known as “long COVID” or “long-haul COVID”.[7,9]
An agreed-upon global definition, post-COVID condition (PCC?), aims to help focus research, clarify terminology for medical use and better define and capture cases of PCC.[9] PCC occurs in those with a history of probable or confirmed SARS-CoV -2 infection, usually three months from illness onset, with symptoms (no minimum number) that last for at least two months and cannot be explained by an alternative diagnosis.[9]
We know that SARS-CoV-2 can travel all over the body and infect a wide range of our cells. But PCC remains unclear, but to many very worrisome black box of unknowns.
Some of the questions still outstanding include:
What proportion of total COVID-19 cases ends up with PCC? What proportion of those with PCC had no symptoms or had a mild, moderate or severe disease course following SARS-CoV-2 infection?
What proportion of those with PCC has a pre-existing or underlying condition?
Does immunity from vaccination prevent, modify or have any impact at all on the number of people who acquire PCC?
What is the impact of vaccination on PCC once you have it?
What else might help treat or manage PCC – from medicines to exercise to vitamins…?
Is the length of PCC affected by age, sex or comorbidities?
Are there any factors that affect the prognosis of those with PCC?
Summary
It does seem that the latest and most ubiquitous variant, Omicron, causes less severe disease compared to the Delta variant.[8,12,13,14] Vaccination – especially after boosting – and prior infection also help to modify disease outcomes further to be less severe [8,13]. Still, PCC casts a shadow that remains a lingering concern to be addressed in this pandemic.
Apart from PCC’s many unknowns, we have entered into the chapter that I’m calling “Living Next Door to Alice” for now. I think it could be one of the last few chapters in this book.
Former Project Veritas & O’Keefe Media Group operative and Pfizer formulation analyst scientist Justin Leslie revealed previously unpublished recordings showing Pfizer’s top vaccine researchers discussing major concerns surrounding COVID-19 vaccines. Leslie delivered these recordings to Veritas in late 2021, but they were never published:
Principal scientist at Pfizer, Kanwall Gill in 2021:
“We had no idea how it’s going to look like. MRNA vaccines have been there for 50 years, but nothing went to clinical trial because MRNA have been known to have side effects.”
Featured in Leslie’s footage is Kanwal Gill, a principal scientist at Pfizer. Gill was weary of MRNA technology given its long research history yet lack of approved commercial products. She called the vaccines “sneaky,” suggesting latent side effects could emerge in time.
Gill goes on to illustrate how the vaccine formulation process was dramatically rushed under the FDA’s Emergency Use Authorization and adds that profit incentives likely played a role:
Pfizer's principal scientist in 2021:
“It takes 10 year for a vaccine to come out. It takes years of observations... we are doing everything at the same time."
"It’s going to affect my heart, and I’m going to die. And nobody’s talking about that."
Leslie recorded another colleague, Pfizer’s pharmaceutical formulation scientist Ramin Darvari, who raised the since-validated concern that repeat booster intake could damage the cardiovascular system:
Pfizer's pharmaceutical formulation scientist, Ramin Darvari, in 2021:
“They’re engineering it specifically for me to take the next one, so increasing my consumption."
“It’s going to affect my heart, and I’m going to die. And nobody’s talking about that.”
None of these claims will be shocking to hear in 2024, but it is telling that high-level Pfizer researchers were discussing these topics in private while the company assured the public of “no serious safety concerns” upon the jab’s release:
Vaccine for Children is a Different Formulation
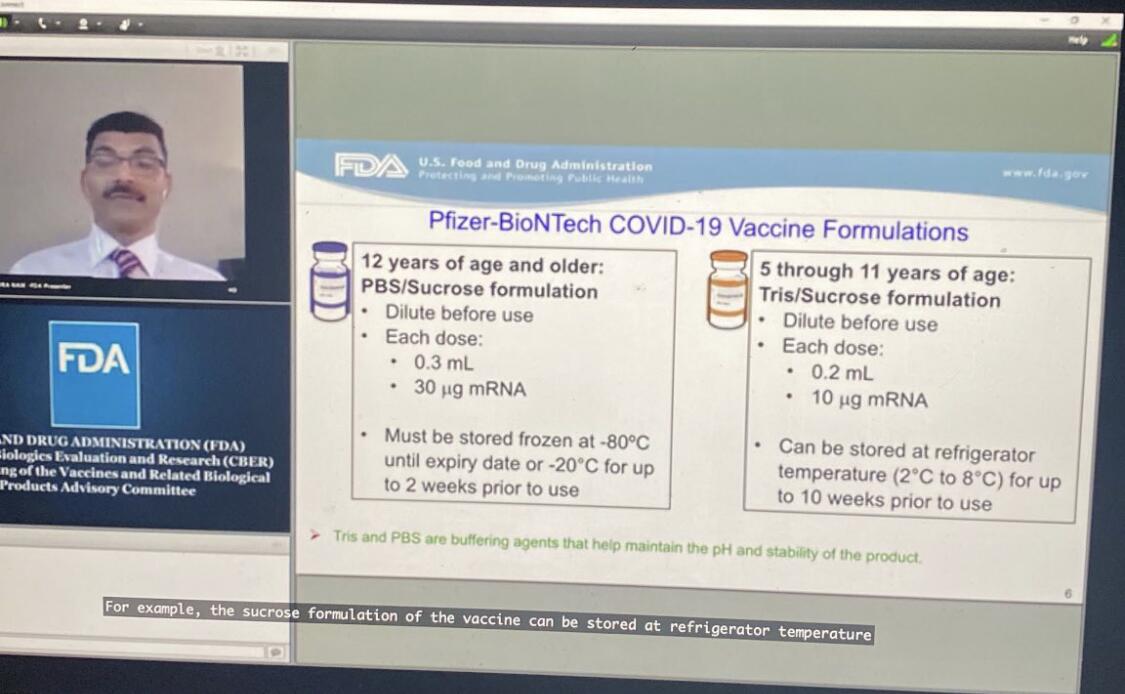
Leslie sent me a little-known FDA-Pfizer conference — a 7-hour Zoom meeting published in tandem with the approval of the vaccine for 5 – 11 year-olds — during which Pfizer’s vice presidents of vaccine research and development, Nicholas Warne and William Gruber, discussed a last-minute change to the vaccine’s “buffer” — from “PBS” to “Tris” — to improve its shelf life. For about 30 seconds of these 7 hours, Gruber acknowledged that the new formula was NOT the one used in clinical trials (emphasis mine):
“The studies were done using the same volume… but contained the PBS buffer. We obviously had extensive consultations with the FDA and it was determined that the clinical studies were not required because, again, the LNP and the MRNA are the same and the behavior — in terms of reactogenicity and efficacy — are expected to be the same.”
According to Leslie, the tweaked “buffer” dramatically changed the temperature needed for storage: “Before they changed this last step of the formulation, the formula was to be kept at -80 degrees Celsius. After they changed the last step, we kept them at 2 to 8 degrees celsius,” Leslie told me.
The claims are backed up in the referenced video presentation:
I’m no vaccinologist but an 80-degree temperature delta — and a 5x shelf-life in a warmer climate — seems like a significant change that might warrant clinical trials before commercial release.
Despite this information technically being public, there has been virtually no media scrutiny or even coverage — and in fact, most were told the vaccine for children was the same formula but just a smaller dose — which is perhaps due to a combination of the information being buried within a 7-hour jargon-filled presentation and our media being totally dysfunctional.
Bohemian Grove?
Leslie’s 2-hour long documentary on his experience at both Pfizer and O’Keefe’s companies concludes on an interesting note: James O’Keefe attended an outing at the Bohemian Grove.
Leslie offers this photo of James’ Bohemian Grove “GATE” slip as evidence, left on his work desk atop a copy of his book, “American Muckraker”:
My thoughts on the Bohemian Grove: my good friend’s dad was its general manager for several decades. From what I have gathered through that connection, the Bohemian Grove is not some version of the Illuminati, at least not in the institutional sense.
Do powerful elites hangout there? Absolutely. Do they discuss their plans for the world while hanging out there? I’m sure it has happened. Do they have a weird ritual with a giant owl? Yep, Alex Jones showed that to the world.
My perspective is based on conversations with my friend and my belief that his father is not lying to him. I could be wrong and am open to evidence — like if boxer Ryan Garcia decides to produce evidence regarding his rape claims — and I do find it a bit strange the club would invite O’Keefe who is notorious for covertly filming, but Occam’s razor would lead me to believe the club is — as it was under my friend’s dad — run by boomer conservatives the extent of whose politics include disliking wokeness, immigration, and Biden (common subjects of O’Keefe’s work).
Therefore, I don’t find O’Keefe’s visit to the club indicative that he is some sort of Operation Mockingbird asset as Leslie tries to depict (however Mockingbird is a 100% legitimate conspiracy). I have also met James several times and even came close to joining OMG. While I disagreed with James on the significance of many of his stories — finding some to be overhyped and showy — I never doubted his conviction in them.
As for why Leslie’s story was squashed… all my sources told me it was to avoid jail time for Veritas executives.
Feel free to watch Leslie’s full documentary here and decide for yourself.
Fun fact — Justin Leslie was also the operative behind this mega-viral Project Veritas story where Pfizer’s director of R&D claimed the company was privately mutating COVID-19 behind closed doors:
BREAKING: @Pfizer Exploring "Mutating" COVID-19 Virus For New Vaccines
"Don't tell anyone this...There is a risk...have to be very controlled to make sure this virus you mutate doesn't create something...the way that the virus started in Wuhan, to be honest."#DirectedEvolutionpic.twitter.com/xaRvlD5qTo
“[…] our findings support the hypothesis that the intrauterine environment, particularly essential and non-essential metals, affect epigenetic aging biomarkers across the life course.”
Credit: 2024 Bozack et al.
“[…] our findings support the hypothesis that the intrauterine environment, particularly essential and non-essential metals, affect epigenetic aging biomarkers across the life course.”
BUFFALO, NY- March 12, 2024 – A new research paper was published inAging (listed by MEDLINE/PubMed as “Aging (Albany NY)” and “Aging-US” by Web of Science) Volume 16, Issue 4, entitled, “Associations of prenatal one-carbon metabolism nutrients and metals with epigenetic aging biomarkers at birth and in childhood in a US cohort.”
Epigenetic gestational age acceleration (EGAA) at birth and epigenetic age acceleration (EAA) in childhood may be biomarkers of the intrauterine environment. In this new study, researchers Anne K. Bozack, Sheryl L. Rifas-Shiman, Andrea A. Baccarelli, Robert O. Wright, Diane R. Gold, Emily Oken, Marie-France Hivert, and Andres Cardenas from Stanford University School of Medicine, Harvard Medical School, Harvard T.H. Chan School of Public Health, Columbia University, and Icahn School of Medicine at Mount Sinai investigated the extent to which first-trimester folate, B12, 5 essential and 7 non-essential metals in maternal circulation are associated with EGAA and EAA in early life.
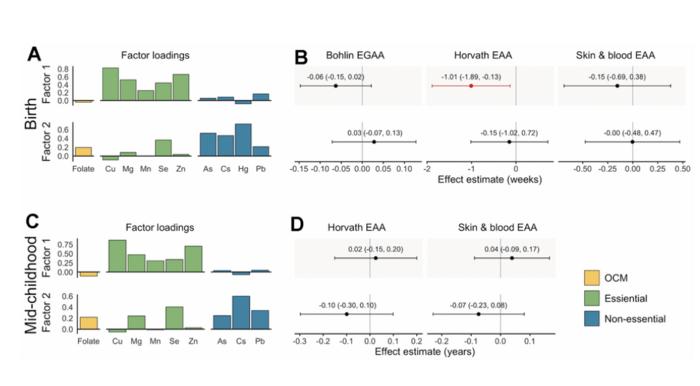
“[…] we hypothesized that OCM [one-carbon metabolism] nutrients and essential metals would be positively associated with EGAA and non-essential metals would be negatively associated with EGAA. We also investigated nonlinear associations and associations with mixtures of micronutrients and metals.”
Bohlin EGAA and Horvath pan-tissue and skin and blood EAA were calculated using DNA methylation measured in cord blood (N=351) and mid-childhood blood (N=326; median age = 7.7 years) in the Project Viva pre-birth cohort. A one standard deviation increase in individual essential metals (copper, manganese, and zinc) was associated with 0.94-1.2 weeks lower Horvath EAA at birth, and patterns of exposures identified by exploratory factor analysis suggested that a common source of essential metals was associated with Horvath EAA. The researchers also observed evidence of nonlinear associations of zinc with Bohlin EGAA, magnesium and lead with Horvath EAA, and cesium with skin and blood EAA at birth. Overall, associations at birth did not persist in mid-childhood; however, arsenic was associated with greater EAA at birth and in childhood.
“Prenatal metals, including essential metals and arsenic, are associated with epigenetic aging in early life, which might be associated with future health.”
Read the full paper: DOI:https://doi.org/10.18632/aging.205602
Corresponding Author: Andres Cardenas
Corresponding Email:andres.cardenas@stanford.edu
Keywords: epigenetic age acceleration, metals, folate, B12, prenatal exposures
Click here to sign up for free Altmetric alerts about this article.
About Aging:
Launched in 2009, Aging publishes papers of general interest and biological significance in all fields of aging research and age-related diseases, including cancer—and now, with a special focus on COVID-19 vulnerability as an age-dependent syndrome. Topics in Aging go beyond traditional gerontology, including, but not limited to, cellular and molecular biology, human age-related diseases, pathology in model organisms, signal transduction pathways (e.g., p53, sirtuins, and PI-3K/AKT/mTOR, among others), and approaches to modulating these signaling pathways.
Please visit our website at www.Aging-US.com and connect with us:
National insurance, income tax, VAT, capital gains tax, inheritance tax… it’s easy to get confused about the many different ways we contribute to the cost of running the country. The budget announcement is the key time each year when the government shares its financial plans with us all, and announces changes that may make a tangible difference to what you pay.
But you’ll likely be hearing a lot more about taxes in the coming months – promises to cut or raise them are an easy win (or lose) for politicians in an election year. We may even get at least one “mini-budget”.
If you’ve recently entered the workforce or the housing market, you may still be wrapping your mind around all of these terms. Here is what you need to know about the different types of taxes and how they affect you.
The UK broadly uses three ways to collect tax:
1. When you earn money
If you are an employee or own a business, taxes are deducted from your salary or profits you make. For most people, this happens in two ways: income tax, and national insurance contributions (or NICs).
If you are self-employed, you will have to pay your taxes via an annual tax return assessment. You might also have to pay taxes this way for interest you earn on savings, dividends (distribution of profits from a company or shares you own) received and most other forms of income not taxed before you get it.
VAT and excise duties are taxes on most goods and services you buy, with some exceptions like books and children’s clothing. About 20% of the total tax collected is VAT.
3. Taxes on wealth and assets
These are mainly taxes on the money you earn if you sell assets (like property or stocks) for more than you bought them for, or when you pass on assets in an inheritance. In the latter case in the UK, the recipient doesn’t pay this, it is the estate paying it out that must cover this if due. These taxes contribute only about 3% to the total tax collected.
You also likely have to pay council tax, which is set by the council you live in based on the value of your house or flat. It is paid by the user of the property, no matter if you own or rent. If you are a full-time student or on some apprenticeship schemes, you may get a deduction or not have to pay council tax at all.
This article is part of Quarter Life, a series about issues affecting those of us in our 20s and 30s. From the challenges of beginning a career and taking care of our mental health, to the excitement of starting a family, adopting a pet or just making friends as an adult. The articles in this series explore the questions and bring answers as we navigate this turbulent period of life.
Put together, these totalled almost £790 billion in 2022-23, which the government spends on public services such as the NHS, schools and social care. The government collects taxes from all sources and sets its spending plans accordingly, borrowing to make up any difference between the two.
Income tax
The amount of income tax you pay is determined by where your income sits in a series of “bands” set by the government. Almost everyone is entitled to a “personal allowance”, currently £12,570, which you can earn without needing to pay any income tax.
You then pay 20% in tax on each pound of income you earn (across all sources) from £12,570-£50,270. You pay 40% on each extra pound up to £125,140 and 45% over this. If you earn more than £100,000, the personal allowance (amount of untaxed income) starts to decrease.
If you are self-employed, the same rates apply to you. You just don’t have an employer to take this off your salary each month. Instead, you have to make sure you have enough money at the end of the year to pay this directly to the government.
The government can increase the threshold limits to adjust for inflation. This tries to ensure any wage rise you get in response to higher prices doesn’t lead to you having to pay a higher tax rate. However, the government announced in 2021 that they would freeze these thresholds until 2026 (extended now to 2028), arguing that it would help repay the costs of the pandemic.
Given wages are now rising for many to help with the cost of living crisis, this means many people will pay more income tax this coming year than they did before. This is sometimes referred to as “fiscal drag” – where lower earners are “dragged” into paying higher tax rates, or being taxed on more of their income.
National insurance
National insurance contributions (NICs) are a second “tax” you pay on your income – or to be precise, on your earned income (your salary). You don’t pay this on some forms of income, including savings or dividends, and you also don’t pay it once you reach state retirement age (currently 66).
While Jeremy Hunt, the current chancellor of the exchequer, didn’t adjust income tax meaningfully in this year’s budget, he did announce a cut to NICs. This was a surprise to many, as we had already seen rates fall from 12% to 10% on incomes higher than £242/week in January. It will now fall again to 8% from April.
While this is charged separately to income tax, in reality it all just goes into one pot with other taxes. Some, including the chancellor, say it is time to merge these two deductions and make this simpler for everyone. In his budget speech this year, Hunt said he’d like to see this tax go entirely. He thinks this isn’t fair on those who have to pay it, as it is only charged on some forms of income and on some workers.
I wouldn’t hold my breath for this to happen however, and even if it did, there are huge sums linked to NICs (nearly £180bn last year) so it would almost certainly have to be collected from elsewhere (such as via an increase in income taxes, or a lot more borrowing) to make sure the government could still balance its books.
There are likely to be further tweaks to the UK’s tax system soon, perhaps by the current government before the election – and almost certainly if there is a change of government.
Wealth taxes may be in line for a change. In the budget, the chancellor reduced capital gains taxes on sales of assets such as second properties (from 28% to 24%). These types of taxes provide only a limited amount of money to the government, as quite high thresholds apply for inheritance tax (up to £1 million if you are passing on a family home).
There are calls from many quarters though to look again at these types of taxes. Wealth inequality (the differences between total wealth held by the richest compared to the poorest) in the UK is very high (much higher than income inequality) and rising.
But how to do this effectively is a matter of much debate. A recent study suggested a one-off tax on total wealth held over a certain threshold might work. But wealth taxes are challenging to make work in practice, and both main political parties have already said this isn’t an option they are considering currently.
Andy Lymer and his colleagues at the Centre for Personal Financial Wellbeing at Aston University currently or have recently received funding for their research work from a variety of funding bodies including the UK's Money and Pension Service, the Aviva Foundation, Fair4All Finance, NEST Insight, the Gambling Commission, Vivid Housing and the ESRC, amongst others.
We use cookies on our website to give you the most relevant experience by remembering your preferences and repeat visits. By clicking “Accept”, you consent to the use of ALL the cookies.
This website uses cookies to improve your experience while you navigate through the website. Out of these, the cookies that are categorized as necessary are stored on your browser as they are essential for the working of basic functionalities of the website. We also use third-party cookies that help us analyze and understand how you use this website. These cookies will be stored in your browser only with your consent. You also have the option to opt-out of these cookies. But opting out of some of these cookies may affect your browsing experience.
Necessary cookies are absolutely essential for the website to function properly. These cookies ensure basic functionalities and security features of the website, anonymously.
Cookie
Duration
Description
cookielawinfo-checbox-analytics
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Analytics".
cookielawinfo-checbox-functional
11 months
The cookie is set by GDPR cookie consent to record the user consent for the cookies in the category "Functional".
cookielawinfo-checbox-others
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Other.
cookielawinfo-checkbox-necessary
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookies is used to store the user consent for the cookies in the category "Necessary".
cookielawinfo-checkbox-performance
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Performance".
viewed_cookie_policy
11 months
The cookie is set by the GDPR Cookie Consent plugin and is used to store whether or not user has consented to the use of cookies. It does not store any personal data.
Functional cookies help to perform certain functionalities like sharing the content of the website on social media platforms, collect feedbacks, and other third-party features.
Performance cookies are used to understand and analyze the key performance indexes of the website which helps in delivering a better user experience for the visitors.
Analytical cookies are used to understand how visitors interact with the website. These cookies help provide information on metrics the number of visitors, bounce rate, traffic source, etc.
Advertisement cookies are used to provide visitors with relevant ads and marketing campaigns. These cookies track visitors across websites and collect information to provide customized ads.













































{kind=link}
{kind=link}