
Researchers Identify Physician and Patient Concerns Around COVID Digital Detection Surveillance in China
To highlight ethical considerations for promoting patients’ autonomy and health care rights, researchers from mainland China, Hong Kong and New Zealand present the results of interviews documenting patient and primary care physicians with digital surveillance of infectious disease (including COVID-19) in urban areas of northern and southern China. The authors conducted in-depth interviews with 16 primary care physicians and 24 of their patients, reflecting a range of ages, educational backgrounds and clinical experiences. Ethical approval was granted by the Institutional Review Board of the University of Hong Kong-Shenzhen Hospital in China.
The team identified five frequently mentioned concerns raised by primary care physicians and patients : 1) ambiguity around the need for informed consent about the usage of digital detection surveillance data; 2) the importance of autonomous decision-making; 3) the potential for discrimination with digital detection surveillance of people who have an infectious disease; 4) the risk of social inequity and divided care outcomes; and 5) authoritarian institutions’ responsibility for maintaining health data security. The adoption of digital detection surveillance meant some patients would be reluctant to go to a hospital for fear of either being discriminated against or forcibly quarantined. Certain groups such as older people and children were thought to be vulnerable to digital detection surveillance data misuse.
The authors argue that in establishing national and international ethical frameworks for digital detection surveillance that protects patients but allows for coordinated management during pandemics, guidelines should include protections against social inequity.
Primary Care Physicians’ and Patients’ Perspectives on Equity and Health Security of Infectious Disease Digital Surveillance
Eleanor Holroyd, PhD, et al
Department of Nursing, School of Clinical Sciences, Auckland University of Technology, Auckland, New Zealand.
Permanent link
Primary Care Plays a Role in Helping Patients With Long COVID Symptoms by Providing Holistic, Trustworthy Care
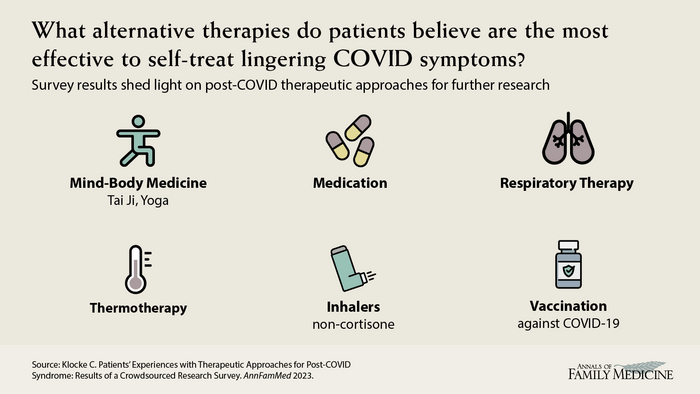
Many people are experiencing a variety of long COVID-19 symptoms and are relying on some of their own methods to allay those symptoms. Others are in need of additional therapies from their medical care team. Researchers from Germany asked patients experiencing post-COVID symptoms about the therapies they used and found effective, as well as their ongoing medical needs. Almost 500 participants completed an online survey about individual experiences with various therapeutic strategies.
The most common symptoms included fatigue, physical exhaustion, difficulty concentrating, and loss of taste and smell. Patient approaches to alleviating symptoms included mind-body medicine, the use of nutritional supplements, sports activities/exercise, and olfactory training in the case of loss of smell. When asked about their specific medical needs, only 13% of patients indicated they had no additional needs. Thirty-five percent of patients wanted more understanding and recognition of their situation and 33% indicated the need for specific post-COVID healthcare services, as well as more information. Additionally, study authors suggest that doctors be more attentive to patient’s needs for empathy and understanding.
Patients’ Experiences With Therapeutic Approaches for Post-COVID Syndrome: Results of a Crowdsourced Research Survey
Carina Klocke, MSc, et al
Institute for General Practice and Interprofessional Care, University Hospital and Faculty of Medicine, Tübingen, Germany
Permanent link
Comprehensive Primary Care, Accessibility and Continuity Can Reduce Hospitalizations
Japanese researchers examined the association between primary care practice characteristics and total hospitalizations during the COVID-19 pandemic. They conducted a nationwide study and examined data from 1,161 participants ages 40-75. They assessed the quality of primary care attributes, including first contact between the patient and a primary care clinician, length of care, care coordination, comprehensiveness and the clinic’s orientation in the community. Researchers primarily sought to identify any hospitalizations among participants during a 12-month period between May 2021 and April 2022.
Each primary care attribute – such as accessibility, continuity, coordination and comprehensiveness – was associated with a reduction in hospitalizations. High-quality primary care was associated with decreased total hospitalizations, even during a pandemic when there are many barriers to providing routine medical care. The authors argued that these findings support policies intended to strengthen primary care systems during and after the COVID-19 pandemic. Theintegration of public health practice with the delivery of primary care services may be a more important process, especially during a pandemic.
Impact of Primary Care Attributes on Hospitalization During the COVID-19 Pandemic: A Nationwide Prospective Cohort Study in Japan
Takuya Aoki, MD, PhD, MMA, et al
Division of Clinical Epidemiology, Research Center for Medical Sciences, The Jikei University School of Medicine, Tokyo, and Section of Clinical Epidemiology, Department of Community Medicine, Graduate School of Medicine, Kyoto University, Kyoto, Japan
Permanent link
Primary Care Practices Implemented More Care Management Processes Despite the Impact of COVID-19
Although primary care clinics were disrupted by the COVID-19 pandemic, a study by Minnesota researchers showed that care management processes for chronic disease care in the primary care setting generally increased from 2019 to 2021. The team used data from 269 primary care clinics in 2017, 2019 and 2021, as well as data from 287 clinics that completed surveys in only one or two years, to learn whether the pandemic’s disruptions compromised health care for people with chronic conditions. Overall care management process scores increased by similar amounts (1.6% and 2.1%) from 2017-2019 and from 2019-2021. However, the score for two care management process areas, specifically performance and management of high-risk patients and hospitalizations, decreased in 2021. Clinics affiliated with larger organizations had higher care management process scores when compared to clinics in smaller organizations. Scores were lower in rural areas compared to urban area clinics. This improvement occurred despite reports from 55% of clinic leaders that the pandemic had been extremely or very disruptive. According to the researchers, increasing highly organized care management practices may be an important step in recovering from losses in health care service quality.
COVID-19 Impacts on Primary Care Clinic Care Management Processes
Leif I. Solberg, MD, et al
HealthPartners Institute, Minneapolis, Minnesota
Permanent link
Also in this Issue
National Research Team Examines Challenges, Responses and Innovations During COVID Pandemic
Investigators have written a special report about the Agency for Healthcare Research and Quality’s learning community, which operated from December 2020-November 2021. It provided a forum for individuals to share learning and gain peer support; to better understand the stressors and challenges confronting practices; to ascertain needs; and to identify promising solutions in response to the COVID-19 pandemic. The engagement of the community provided valuable insights that can inform future research and policy; identify primary care delivery improvements; and ensure that the primary care community is better prepared to respond and contribute to ongoing and future health challenges.
Primary Care’s Challenges and Responses in the Face of the COVID-19 Pandemic: Insights From AHRQ’s Learning Community
Sebastian T. Tong, MD, MPH, et al
University of Washington, Seattle, Washington and Center for Evidence and Practice Improvement, Agency for Healthcare Research and Quality, Rockville, Maryland
Permanent link
Academic and Public Health Partnership Creates Data Bridge to Promote Information Sharing During COVID-19 Pandemic
Clinicians and administrators in Alberta, Canada, built a data bridge between primary care and public health stakeholders to improve the province’s community-based response to the pandemic. The authors traced the data bridge’s foundations to: policy commitments to the Patient Medical Home model as well as organizational and governance structures that actively drew together primary care and non-primary care stakeholders. Those commitments and structures opened the possibility for champions to emerge, trust to evolve, and integrative improvisation of health care practices to take place. Without a functional and well-established interface between independent primary care and the central health system, the authors argue that both pandemic responses, and everyday primary care integration efforts are likely to suffer.
Building a Data Bridge: Policies, Structures, and Governance Integrating Primary Care Into the Public Health Response to COVID-19
Myles Leslie, PhD, MJ, MA, et al
School of Public Policy and Cumming School of Medicine, Department of Community Health Sciences, University of Calgary, Alberta, Canada
Permanent link
Community Health Information Exchanges May Reduce Likelihood of Re-hospitalizations and Follow-up Emergency Department Visits
Researchers examined whether primary care physicians’ use of a secure community health information exchange (HIE) to access data about patient care transitions reduced the likelihood of the patient being re-hospitalized. Doctors’ use of the HIE was associated with an increased length of time that patients were admitted to the ED from 99 to 238 days. The likelihood of a return visit to the ED was decreased by 53% while re-hospitalization decreased by 61%.
The Impact of Community Health Information Exchange Usage on Time to Reutilization of Hospital Services
Chantel Sloan-Aagard, PhD, et al
Paso del Norte Health Information Exchange, El Paso, Texas, and the Department of Public Health, Brigham Young University, Provo, Utah
Permanent link
Study Suggests Primary Care Clinical Staff and Patients Prefer Self-Rooming During COVID-19 Pandemic
During the COVID-19 pandemic, clinic staff have had to adjust the ways in which they see patients in person so that they remain safe. Researchers conducted a study to determine patient and staff perceptions of a process that allowed patients, after check-in, to find their own exam rooms. Most of the 1,561 patients surveyed in this study preferred self-rooming, especially among patients aged 65 years and younger and in family medicine clinics. Few patients said they felt less welcomed, less cared about, more isolated, more lost or confused, or more frustrated with self-rooming compared to escorted-rooming. Over half of staff preferred self-rooming and thought most patients did as well.
Primary Care Patients’ and Staff’s Perceptions of Self-Rooming as Alternative to Waiting Rooms
Edmond Ramly, PhD, et al
Department of Family Medicine and Community Health, University of Wisconsin School of Medicine and Public Health, Primary Care Academics Transforming Healthcare Collaborative, UW Health, Madison, Wisconsin
Permanent link
Insulin Underuse in Primary Care Requires Clinicians to Remove Barriers to Patient Access
The rising cost of insulin has created problems in diabetes management. Researchers conducted a survey study to determine the prevalence of cost-related insulin underuse in a primary care environment. They examined the frequency of cost-related underuse of insulin within a year of a patient being diagnosed with diabetes. Ninety respondents completed the survey. Among those who completed the survey, 44% experienced cost-related substandard therapy. Participants who reported underuse were approximately nine times more likely to have difficulty purchasing diabetes supplies than those who did not report underuse. However, the majority of respondents experiencing cost-related issues said they discussed it with their prescribers, which significantly increased the likelihood of their doctor changing their insulin. Participants experiencing poor diabetes control were not more likely to report underuse. The authors recommend that primary care physicians use empathy when asking about cost barriers as some patients may be reluctant to speak up about their challenges in obtaining insulin.
A Survey Snapshot Measuring Insulin in Underuse in a Primary Care Clinic
Rick Hess, PharmD, CDCES, BCACP, et al
Department of Pharmacy Practice, Bill Gatton College of Pharmacy, East Tennessee State University, Johnson City, Tennessee
Permanent link
Tool for UTI Detection Performs Well in Primary Care Setting, May Reduce Unnecessary Antibiotics Use
Urinary tract infections (UTI) are commonly diagnosed and treated in primary care. The gold standard for diagnosing a UTI is a urine culture. However, waiting for culture results delays treatment, so doctors often prescribe antibiotics while awaiting those results. Researchers modified a UTI detection algorithm developed and validated in an emergency room population to be usable in a primary care setting. The main modification was removing the requirements for microscopy since results are often not available in primary care. Researchers found that the removal of microscopy features did not severely compromise performance of the UTI detection algorithm in emergency department patients. Additionally, the algorithm performed well in the primary care sample. Results suggest that the new algorithm could be used to safely withhold antibiotics in low risk patients, thereby reducing antibiotic overuse.
Adaptation and External Validation of Pathogenic Urine Culture Prediction in Primary Care Using Machine Learning
Daniel J. Parente, MD, PhD, et al
Department of Family Medicine and Community Health University of Kansas Medical Center, Kansas City, Kansas
Permanent link
“The Trust Circle” Promotes Inclusion of American Indian and Alaska Native Populations in Clinical Trials
Indigenous populations, including people of American Indian and Alaska Native origin, are underrepresented in clinical trials. Researchers collaborated to modify the “trust triangle” model used in clinical trial recruitment and expanded it to a new model called, “The Trust Circle.” This new model takes into account the various entities that are part of the recruitment process and the trust that must be developed between trial participants, researchers and other individuals such as physicians, ministers and community leaders. The authors assert that physicians, ministers and community leaders can promote trust and assist in the recruitment of AI/AN populations to clinical trials. This in turn can promote health improvement of these populations.
Recruiting Indigenous Patients Into Clinical Trials: A Circle of Trust
Arch G. Mainous III, PhD, et al
Department of Community Health and Family Medicine and Department of Health Services Research Management, and Policy, University of Florida, Gainesville, Florida
Permanent link
Despite Benefits, Use of Clinical Decision Support Systems is Curbed by Workload Challenges
French researchers conducted a systematic review of qualitative, quantitative and mixed methods studies to identify and quantify the barriers and facilitators primary care providers (PCPs) experience when using clinical decision support systems (CDSSs) – software designed to facilitate clinical decision-making. The greatest barrier to using CDSSs was an increased workload through use of CDSS. Human and organizational factors also had negative impacts on CDSS use, whereas technological factors had a neutral impact. The net benefits dimension of the Human Organization Technology framework the authors used to study the barriers and facilitators had a positive impact, including CDSSs’ potential to improve quality of care, particularly for preventive care. Although PCPs find benefit from and support the potential effectiveness of CDSSs in improving the quality and safety of care, they also highlight their lack of efficiency due to increased workload. The authors concluded that CDSS developers need to better address human and organizational issues, in addition to technological challenges. They also proposed a list of 11 features of CDSSs expected to improve their usability in primary care.
Barriers and Facilitators to the Use of Clinical Decision Support Systems in Primary Care: A Mixed-Methods Systematic Review
Pierre-Yves Meunier, MD, et al
Collège Universitaire de Médecine Générale and Research on Healthcare Performance (RESHAPE), Université Claude Bernard Lyon 1, Lyon, France
Permanent link
Editorial: While Key to Pandemic Response, Primary Care Could Not Overcome Socioeconomic Inequities and Reduction in Care-Seeking Behaviors
Trisha Greenhalgh, MD, professor of primary health care sciences and co-director of Interdisciplinary Research In Health Sciences at the University of Oxford, writes the editorial in this edition of Annals of Family Medicine. She mentions the numerous papers in this edition that explain the ways in which primary care members in various countries surveilled the virus; bridged information gaps; managed patient care and clinical practices; and in general, affected health outcomes in individuals affected by the COVID pandemic. From the patient perspective, researchers also studied how people affected by COVID managed long-term symptoms themselves. Greenhalgh adds that primary care contributes to overall health system resilience. She also challenges primary care clinicians to continue fighting for the resources they need to restore the existing workforce, incentivize the next generation of primary care providers, and defend the core values that underpin the field’s critical work with individuals, families and communities.
Covid-19 and Primary Care: Taking Stock
Professor Trisha Greenhalgh, MD
University of Oxford, Oxford, England
Permanent link
Primary Care Doctor Who Experienced Hacking Outlines Strategies for Preventing Online Attacks
Ed Bujold, MD, a family medicine doctor, writes about his solo practice being attacked by ransomware. He describes how he was able to get his practice back in operating order and offers recommendations to other primary care practices in protecting themselves from potential hackers.
You Have Been Hacked!
Ed Bujold, MD, FAAFP
Family Medical Care Center, Granite Falls, North Carolina
Permanent link
Medical Doctor Writes a Letter to her Unborn Daughter About Importance of Abortion Access and Bodily Autonomy
While pregnant with her first child, Laura Krinsky, MD, writes a letter to her daughter about the experience of providing abortions in Massachusetts (a state that has protected abortion access) and Tennessee (a state that has restricted abortion access). In light of the U.S. Supreme Court overturning the constitutional right to abortion, Krinsky writes that she hopes to raise her daughter to be compassionate and humble, to care about people and to respect their bodily autonomy and their health care decisions.
On Abortion and Autonomy: A Letter to My Unborn Daughter
Laura Krinsky MD
Cambridge Health Alliance, Malden, Massachusetts
Permanent link
# # #
Annals of Family Medicine is a peer-reviewed, indexed research journal that provides a cross-disciplinary forum for new, evidence-based information affecting the primary care disciplines. Launched in May 2003, Annals is sponsored by seven family medical organizations, including the American Academy of Family Physicians, the American Board of Family Medicine, the Society of Teachers of Family Medicine, the Association of Departments of Family Medicine, the Association of Family Medicine Residency Directors, the North American Primary Care Research Group, and The College of Family Physicians of Canada. Annals is published six times each year and contains original research from the clinical, biomedical, social and health services areas, as well as contributions on methodology and theory, selected reviews, essays and editorials. Complete editorial content and interactive discussion groups for each published article can be accessed free of charge on the journal’s website, www.AnnFamMed.org.
Journal
The Annals of Family Medicine













































{kind=link}