Government
FDA Adviser Explains Why He Abstained From Vote On Pfizer’s COVID-19 Vaccine For Kids
FDA Adviser Explains Why He Abstained From Vote On Pfizer’s COVID-19 Vaccine For Kids
Authored by Zachary Stieber via The Epoch Times,
The only Food and Drug Administration vaccine advisory panel member to abstain from a major vote this…
Share this:


Authored by Zachary Stieber via The Epoch Times,
The only Food and Drug Administration vaccine advisory panel member to abstain from a major vote this week that essentially authorized Pfizer’s COVID-19 vaccine for children as young as 5 said he did so because of limited safety and efficacy data.
All 17 others voted to advise the administration, or the FDA, to authorize the jab for children between the ages of 5 and 11. The agency already supported doing so and is expected to formalize the authorization soon. The Centers for Disease Control and Prevention would then decide which children should get the shot.
The vote was preceded by nearly eight hours of discussions and presentations, with multiple members expressing concern about the scant data on how the vaccine will affect the age group.
But Dr. Michael Kurilla, an expert on infectious diseases and pathology who directs a division inside the National Institutes of Health, was the only one who didn’t support the recommendation.
Kurilla told The Epoch Times in an email that he opposed the specific, binary wording of the question, which opens up the possibility that any child between 5 and 11 will be able to get the Pfizer vaccine. He was also concerned about the longest follow-up for the clinical trial involving the age group being only three months, data that shows children experience severe cases of COVID-19 much less often than adults, and how a large chunk of them have already had the disease, giving them some level of immunity.
If the authorization goes through as expected, at least some of the age group will be able to get two doses of 10 micrograms each, spaced three weeks apart.
The same dosage interval, with a dosage level three times as high, is currently in place for adults. But adults have seen waning effectiveness, especially against infection, prompting the recent authorization of booster doses.
Because the interval is the same, it can be predicted that the effectiveness will also wane in children, Kurilla said. The lower dosage level, meanwhile, brings into question whether the protection against severe disease and hospitalization will be as strong as in adults.
“Real-world evidence involving adults suggest the 3-week dosing interval is suboptimal in terms of durability and is likely to be similar in children, leading to waning immunity within 4–6 months,” Kurilla said.
“Because the Pfizer vaccine offers protection against serious disease even after antibody titers have waned, there is some other basis for immunity, but at the lower dose in children, there is no expectation that those same immune processes will behave similarly to the higher adult dose.”
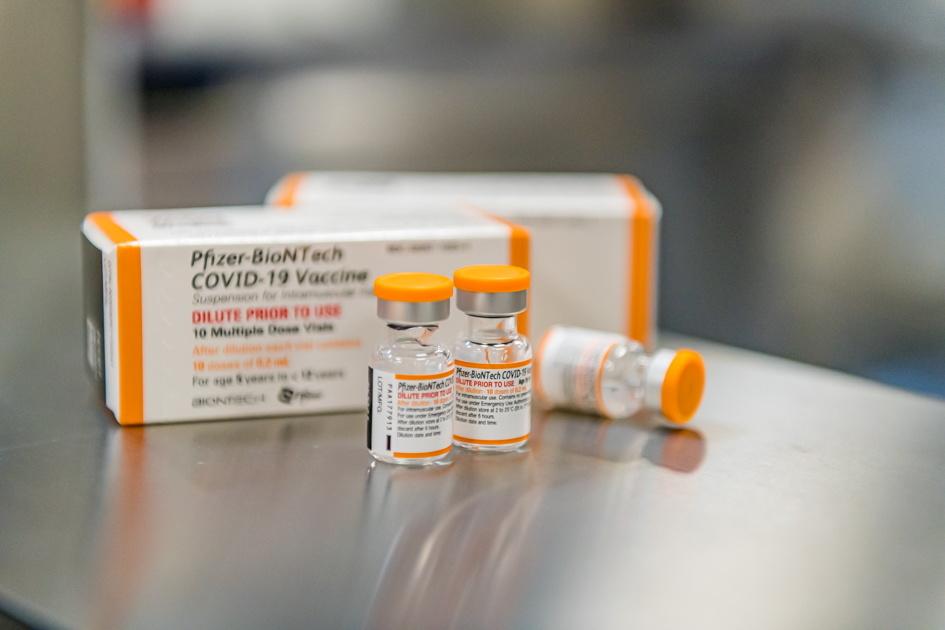
Pfizer/BioNTech’s new pediatric COVID-19 vaccine vials are seen in this undated handout photo. (Pfizer via Reuters)
Low Hospitalization Rate
During the meeting, members heard that among children 5 to 11 in the United States, there have been over 1.9 million infections since the start of the pandemic, but just 0.4 percent, or 8,400 of those cases, have required hospital care. And just 94 of them ended up dying.
They also heard that an estimated 20 percent of the hospitalized children were admitted for a reason besides COVID-19 and that nearly seven out of 10 of the children had existing serious health conditions like heart disease, illustrating just how little risk COVID-19 poses to healthy children.
Further, the Centers for Disease Control and Prevention (CDC) estimates that 40 percent of children in the age group have already had COVID-19. Recovery from COVID-19 bestows some level of immunity, studies show, with multiple studies indicating the level is actually higher than vaccines provide.
“The benefit here is assumed to be prevention of severe disease, which is what we’re all hoping for,” Kurilla said during the meeting.
But among the recovered, he added later, “The question really becomes, does this vaccine offer any benefits to them at all?”
Kurilla signaled he would have voted “yes” if the FDA had proposed opening up access to the vaccine to a subset of the 5–11 group. He also explained why he abstained.
“My abstention was based on the specific question the FDA asked. A ‘no’ vote would have been misconstrued as my opinion about the vaccine,” he told The Epoch Times. “There are high-risk groups within the 5–11 age group that would benefit from the vaccine, suggesting a more tailored approach.”

In this image from video, Dr. Michael Kurilla (C) questions the CDC’s Dr. Fiona Havers (R) during an FDA advisory panel meeting on Oct. 26, 2021. (The Epoch Times via FDA)
Others Question Widespread Use
Additional panel members openly questioned whether all young children should get the vaccine.
“I’m torn. On one hand, we know that many mothers and fathers and parents are eager to administer this vaccine to children because they’re so frightened, perhaps overly so, … that they really are anticipating having access to this vaccine in children,” said Dr. Cody Meissner, the director of pediatric infectious disease at Tufts Medical Center.
“On the other hand, I think we saw that approximately 68 percent of the children who are hospitalized with COVID-19 have underlying comorbidities. That means about 32 percent do not. And then if we were to take 40 percent of that group that may have immunity already, we’re getting down to a very small percent of otherwise healthy 6- to 11-year-old children who might derive some benefit,” he added.
But others said they saw the need for the vaccination. The protection it gives would prevent more hospitalizations and ensure schools remain open, some argued.
“We don’t want children to be dying of COVID, even if it is far fewer children than adults, and we don’t want them in the ICU,” said Dr. Amanda Cohn, a CDC official.
Jeannette Lee, a biostatistics professor at the University of Arkansas for Medical Sciences, said she was impressed by the data presented by Pfizer, which relied on an approach called immunobridging. In this case, Pfizer’s trial showed the vaccine triggered antibodies in children. The antibodies were compared to those elicited in older groups, and that was used as proof the vaccine will protect the kids against COVID-19.
Kurilla, though, voiced disapproval with the approach, telling colleagues “it’s being based on an immunogenicity marker that we know wanes.”
He said he hoped for more flexibility in the authorization, including a single dose for some children and no doses for others, based on factors like prior infection.
“There are high-risk individuals and I think they do need to be attended to, that we do need to provide a vaccine for them. But for many others, one dose—or no dose, even, if they’ve had prior COVID infection. I think they may not need anything more,” he said.

A 14-year-old girl gets a Pfizer COVID-19 vaccine in Hartford, Conn., on May 13, 2021. (Joseph Prezioso/AFP via Getty Images)
Side Effects
Cases of heart inflammation after receipt of the Pfizer and Moderna vaccines are highest in youth, especially boys in their teens. Based on reports submitted to the federally run Vaccine Adverse Event Reporting System (VAERS), the cases are higher than expected in males aged 12 to 49 after the second Pfizer dose and females 12 to 24 after the second Pfizer dose.
Over half of the children with confirmed myocarditis or pericarditis studied in the Vaccine Safety Datalink surveillance system required hospital care, though no post-vaccination deaths due to the conditions have been confirmed, according to federal authorities.
Pfizer said none of the 5- to 11-year-olds in its trials experienced post-vaccination heart inflammation. Using a third of the amount of that given to older people is, in part, an attempt to curb side effects, though how that will ultimately turn out is unknown.
FDA scientists said they determined the vaccine would prevent more COVID-19 cases, hospitalizations, and deaths among the age group than vaccine-linked heart inflammation cases, hospitalizations, and deaths. They assumed a vaccine efficacy of 70 percent against COVID-19 cases and an efficacy of 80 percent against hospitalizations linked to the disease. Among young males, “the benefits appear to outweigh the risks,” Hong Yang, an FDA scientist, told members. Among young females, “the benefits clearly outweigh the risks,” she added.
“What will the actual myocarditis rate be in these younger kids?” Dr. Ofer Levy, director of the Precision Vaccines Program at Boston Children’s Hospital, wondered. That group “may be less susceptible to myocarditis, but right now that’s a speculation,” he added. “We don’t know that for sure.”
Members of the public also expressed concern, arguing the safety data wasn’t sufficient to authorize the vaccine for children so young.
But other members pointed to the trial data, the fact fewer reports have come in for 12- to 15-year-olds than 16- and 17-year-olds, and how, generally, fewer younger children experience heart inflammation versus older ones.
“I am not as concerned about myocarditis in this age group as I am in the older kids,” Dr. Melinda Wharton, another CDC official, said.
Surveillance systems like VAERS will help detect if inflammation becomes an issue in the younger children, members said.
“If the surveillance systems do start seeing severe outcomes and deaths from vaccination, I’m quite confident that those surveillance systems will tell us that we need to pause like we did with the J&J vaccine to really have a good idea of what the effects are vaccinating this age group,” said Dr. Patrick Moore, professor at the University of Pittsburgh Cancer Institute.
In this image from video, Dr. Eric Rubin (L) explains why he will vote to advise the FDA to authorize Pfizer’s COVID-19 vaccine for young children during an FDA advisory panel meeting on Oct. 26, 2021. (The Epoch Times via FDA)
The ‘Yes’ Votes
Ultimately, most members said the benefits and predicted benefits of the vaccine in the 5- to 11-year-olds outweighed the risks and potential risks.
“I think this vaccine will likely be effective in reducing pediatric COVID in this age group and may also help reduce transmission. On the safety end, I’m encouraged by the lower dose, … finding a dose that’s immunogenic and had not too much in terms of reactogenicity,” said Dr. Ofer Levy, director of the Precision Vaccines Program at Boston Children’s Hospital.
Dr. Eric Rubin, an adjunct professor at the Harvard TH Chan School of Public Health, said he wanted to give parents the choice to vaccinate their kids, imagining he had a child who was a transplant recipient, though he joined others in saying there are probably some younger children who shouldn’t get the vaccine.
“The question of how broadly to use it, though, I think is a substantial one. And I know it’s not our question, but I—and I know we’re kind of punting that to [the CDC’s advisory panel]—but I do think that it’s a relatively close call,” he said.
Soon after, in a comment that was widely distributed online, he added: “We’re never going to learn about how safe this vaccine is unless we start giving it. That’s just the way it goes. That’s how we found out about rare complications of other vaccines, like the rotavirus vaccine.”
Rubin told The Epoch Times in an email, responding to critics: “The clinical trial of the Pfizer-BioNTech COVID-19 vaccine in children showed no adverse events. All data to date indicate that it is safe. It will prevent the hospitalization of children with severe disease, as it does with adults. The vaccine works, and saves lives.”
International
Illegal Immigrants Leave US Hospitals With Billions In Unpaid Bills
Illegal Immigrants Leave US Hospitals With Billions In Unpaid Bills
By Autumn Spredemann of The Epoch Times
Tens of thousands of illegal…
Share this:


By Autumn Spredemann of The Epoch Times
Tens of thousands of illegal immigrants are flooding into U.S. hospitals for treatment and leaving billions in uncompensated health care costs in their wake.

The House Committee on Homeland Security recently released a report illustrating that from the estimated $451 billion in annual costs stemming from the U.S. border crisis, a significant portion is going to health care for illegal immigrants.
With the majority of the illegal immigrant population lacking any kind of medical insurance, hospitals and government welfare programs such as Medicaid are feeling the weight of these unanticipated costs.
Apprehensions of illegal immigrants at the U.S. border have jumped 48 percent since the record in fiscal year 2021 and nearly tripled since fiscal year 2019, according to Customs and Border Protection data.
Last year broke a new record high for illegal border crossings, surpassing more than 3.2 million apprehensions.
And with that sea of humanity comes the need for health care and, in most cases, the inability to pay for it.
In January, CEO of Denver Health Donna Lynne told reporters that 8,000 illegal immigrants made roughly 20,000 visits to the city’s health system in 2023.
The total bill for uncompensated care costs last year to the system totaled $140 million, said Dane Roper, public information officer for Denver Health. More than $10 million of it was attributed to “care for new immigrants,” he told The Epoch Times.
Though the amount of debt assigned to illegal immigrants is a fraction of the total, uncompensated care costs in the Denver Health system have risen dramatically over the past few years.
The total uncompensated costs in 2020 came to $60 million, Mr. Roper said. In 2022, the number doubled, hitting $120 million.
He also said their city hospitals are treating issues such as “respiratory illnesses, GI [gastro-intenstinal] illnesses, dental disease, and some common chronic illnesses such as asthma and diabetes.”
“The perspective we’ve been trying to emphasize all along is that providing healthcare services for an influx of new immigrants who are unable to pay for their care is adding additional strain to an already significant uncompensated care burden,” Mr. Roper said.
He added this is why a local, state, and federal response to the needs of the new illegal immigrant population is “so important.”
Colorado is far from the only state struggling with a trail of unpaid hospital bills.

Dr. Robert Trenschel, CEO of the Yuma Regional Medical Center situated on the Arizona–Mexico border, said on average, illegal immigrants cost up to three times more in human resources to resolve their cases and provide a safe discharge.
“Some [illegal] migrants come with minor ailments, but many of them come in with significant disease,” Dr. Trenschel said during a congressional hearing last year.
“We’ve had migrant patients on dialysis, cardiac catheterization, and in need of heart surgery. Many are very sick.”
He said many illegal immigrants who enter the country and need medical assistance end up staying in the ICU ward for 60 days or more.
A large portion of the patients are pregnant women who’ve had little to no prenatal treatment. This has resulted in an increase in babies being born that require neonatal care for 30 days or longer.
Dr. Trenschel told The Epoch Times last year that illegal immigrants were overrunning healthcare services in his town, leaving the hospital with $26 million in unpaid medical bills in just 12 months.
ER Duty to Care
The Emergency Medical Treatment and Labor Act of 1986 requires that public hospitals participating in Medicare “must medically screen all persons seeking emergency care … regardless of payment method or insurance status.”
The numbers are difficult to gauge as the policy position of the Centers for Medicare & Medicaid Services (CMS) is that it “will not require hospital staff to ask patients directly about their citizenship or immigration status.”
In southern California, again close to the border with Mexico, some hospitals are struggling with an influx of illegal immigrants.
American patients are enduring longer wait times for doctor appointments due to a nursing shortage in the state, two health care professionals told The Epoch Times in January.
A health care worker at a hospital in Southern California, who asked not to be named for fear of losing her job, told The Epoch Times that “the entire health care system is just being bombarded” by a steady stream of illegal immigrants.
“Our healthcare system is so overwhelmed, and then add on top of that tuberculosis, COVID-19, and other diseases from all over the world,” she said.

A newly-enacted law in California provides free healthcare for all illegal immigrants residing in the state. The law could cost taxpayers between $3 billion and $6 billion per year, according to recent estimates by state and federal lawmakers.
In New York, where the illegal immigration crisis has manifested most notably beyond the southern border, city and state officials have long been accommodating of illegal immigrants’ healthcare costs.
Since June 2014, when then-mayor Bill de Blasio set up The Task Force on Immigrant Health Care Access, New York City has worked to expand avenues for illegal immigrants to get free health care.
“New York City has a moral duty to ensure that all its residents have meaningful access to needed health care, regardless of their immigration status or ability to pay,” Mr. de Blasio stated in a 2015 report.
The report notes that in 2013, nearly 64 percent of illegal immigrants were uninsured. Since then, tens of thousands of illegal immigrants have settled in the city.
“The uninsured rate for undocumented immigrants is more than three times that of other noncitizens in New York City (20 percent) and more than six times greater than the uninsured rate for the rest of the city (10 percent),” the report states.
The report states that because healthcare providers don’t ask patients about documentation status, the task force lacks “data specific to undocumented patients.”
Some health care providers say a big part of the issue is that without a clear path to insurance or payment for non-emergency services, illegal immigrants are going to the hospital due to a lack of options.
“It’s insane, and it has been for years at this point,” Dana, a Texas emergency room nurse who asked to have her full name omitted, told The Epoch Times.
Working for a major hospital system in the greater Houston area, Dana has seen “a zillion” migrants pass through under her watch with “no end in sight.” She said many who are illegal immigrants arrive with treatable illnesses that require simple antibiotics. “Not a lot of GPs [general practitioners] will see you if you can’t pay and don’t have insurance.”
She said the “undocumented crowd” tends to arrive with a lot of the same conditions. Many find their way to Houston not long after crossing the southern border. Some of the common health issues Dana encounters include dehydration, unhealed fractures, respiratory illnesses, stomach ailments, and pregnancy-related concerns.
“This isn’t a new problem, it’s just worse now,” Dana said.

Medicaid Factor
One of the main government healthcare resources illegal immigrants use is Medicaid.
All those who don’t qualify for regular Medicaid are eligible for Emergency Medicaid, regardless of immigration status. By doing this, the program helps pay for the cost of uncompensated care bills at qualifying hospitals.
However, some loopholes allow access to the regular Medicaid benefits. “Qualified noncitizens” who haven’t been granted legal status within five years still qualify if they’re listed as a refugee, an asylum seeker, or a Cuban or Haitian national.
Yet the lion’s share of Medicaid usage by illegal immigrants still comes through state-level benefits and emergency medical treatment.
A Congressional report highlighted data from the CMS, which showed total Medicaid costs for “emergency services for undocumented aliens” in fiscal year 2021 surpassed $7 billion, and totaled more than $5 billion in fiscal 2022.
Both years represent a significant spike from the $3 billion in fiscal 2020.
An employee working with Medicaid who asked to be referred to only as Jennifer out of concern for her job, told The Epoch Times that at a state level, it’s easy for an illegal immigrant to access the program benefits.
Jennifer said that when exceptions are sent from states to CMS for approval, “denial is actually super rare. It’s usually always approved.”
She also said it comes as no surprise that many of the states with the highest amount of Medicaid spending are sanctuary states, which tend to have policies and laws that shield illegal immigrants from federal immigration authorities.
Moreover, Jennifer said there are ways for states to get around CMS guidelines. “It’s not easy, but it can and has been done.”
The first generation of illegal immigrants who arrive to the United States tend to be healthy enough to pass any pre-screenings, but Jennifer has observed that the subsequent generations tend to be sicker and require more access to care. If a family is illegally present, they tend to use Emergency Medicaid or nothing at all.
The Epoch Times asked Medicaid Services to provide the most recent data for the total uncompensated care that hospitals have reported. The agency didn’t respond.
Continue reading over at The Epoch Times
International
Fuel poverty in England is probably 2.5 times higher than government statistics show
The top 40% most energy efficient homes aren’t counted as being in fuel poverty, no matter what their bills or income are.
Share this:


The cap set on how much UK energy suppliers can charge for domestic gas and electricity is set to fall by 15% from April 1 2024. Despite this, prices remain shockingly high. The average household energy bill in 2023 was £2,592 a year, dwarfing the pre-pandemic average of £1,308 in 2019.
The term “fuel poverty” refers to a household’s ability to afford the energy required to maintain adequate warmth and the use of other essential appliances. Quite how it is measured varies from country to country. In England, the government uses what is known as the low income low energy efficiency (Lilee) indicator.
Since energy costs started rising sharply in 2021, UK households’ spending powers have plummeted. It would be reasonable to assume that these increasingly hostile economic conditions have caused fuel poverty rates to rise.
However, according to the Lilee fuel poverty metric, in England there have only been modest changes in fuel poverty incidence year on year. In fact, government statistics show a slight decrease in the nationwide rate, from 13.2% in 2020 to 13.0% in 2023.
Our recent study suggests that these figures are incorrect. We estimate the rate of fuel poverty in England to be around 2.5 times higher than what the government’s statistics show, because the criteria underpinning the Lilee estimation process leaves out a large number of financially vulnerable households which, in reality, are unable to afford and maintain adequate warmth.

Energy security
In 2022, we undertook an in-depth analysis of Lilee fuel poverty in Greater London. First, we combined fuel poverty, housing and employment data to provide an estimate of vulnerable homes which are omitted from Lilee statistics.
We also surveyed 2,886 residents of Greater London about their experiences of fuel poverty during the winter of 2022. We wanted to gauge energy security, which refers to a type of self-reported fuel poverty. Both parts of the study aimed to demonstrate the potential flaws of the Lilee definition.
Introduced in 2019, the Lilee metric considers a household to be “fuel poor” if it meets two criteria. First, after accounting for energy expenses, its income must fall below the poverty line (which is 60% of median income).
Second, the property must have an energy performance certificate (EPC) rating of D–G (the lowest four ratings). The government’s apparent logic for the Lilee metric is to quicken the net-zero transition of the housing sector.
In Sustainable Warmth, the policy paper that defined the Lilee approach, the government says that EPC A–C-rated homes “will not significantly benefit from energy-efficiency measures”. Hence, the focus on fuel poverty in D–G-rated properties.
Generally speaking, EPC A–C-rated homes (those with the highest three ratings) are considered energy efficient, while D–G-rated homes are deemed inefficient. The problem with how Lilee fuel poverty is measured is that the process assumes that EPC A–C-rated homes are too “energy efficient” to be considered fuel poor: the main focus of the fuel poverty assessment is a characteristic of the property, not the occupant’s financial situation.
In other words, by this metric, anyone living in an energy-efficient home cannot be considered to be in fuel poverty, no matter their financial situation. There is an obvious flaw here.
Around 40% of homes in England have an EPC rating of A–C. According to the Lilee definition, none of these homes can or ever will be classed as fuel poor. Even though energy prices are going through the roof, a single-parent household with dependent children whose only income is universal credit (or some other form of benefits) will still not be considered to be living in fuel poverty if their home is rated A-C.
The lack of protection afforded to these households against an extremely volatile energy market is highly concerning.
In our study, we estimate that 4.4% of London’s homes are rated A-C and also financially vulnerable. That is around 171,091 households, which are currently omitted by the Lilee metric but remain highly likely to be unable to afford adequate energy.
In most other European nations, what is known as the 10% indicator is used to gauge fuel poverty. This metric, which was also used in England from the 1990s until the mid 2010s, considers a home to be fuel poor if more than 10% of income is spent on energy. Here, the main focus of the fuel poverty assessment is the occupant’s financial situation, not the property.
Were such alternative fuel poverty metrics to be employed, a significant portion of those 171,091 households in London would almost certainly qualify as fuel poor.
This is confirmed by the findings of our survey. Our data shows that 28.2% of the 2,886 people who responded were “energy insecure”. This includes being unable to afford energy, making involuntary spending trade-offs between food and energy, and falling behind on energy payments.
Worryingly, we found that the rate of energy insecurity in the survey sample is around 2.5 times higher than the official rate of fuel poverty in London (11.5%), as assessed according to the Lilee metric.
It is likely that this figure can be extrapolated for the rest of England. If anything, energy insecurity may be even higher in other regions, given that Londoners tend to have higher-than-average household income.
The UK government is wrongly omitting hundreds of thousands of English households from fuel poverty statistics. Without a more accurate measure, vulnerable households will continue to be overlooked and not get the assistance they desperately need to stay warm.
Torran Semple receives funding from Engineering and Physical Sciences Research Council (EPSRC) grant EP/S023305/1.
John Harvey does not work for, consult, own shares in or receive funding from any company or organisation that would benefit from this article, and has disclosed no relevant affiliations beyond their academic appointment.
european uk pandemicGovernment
Looking Back At COVID’s Authoritarian Regimes
After having moved from Canada to the United States, partly to be wealthier and partly to be freer (those two are connected, by the way), I was shocked,…
Share this:

{kind=link}

After having moved from Canada to the United States, partly to be wealthier and partly to be freer (those two are connected, by the way), I was shocked, in March 2020, when President Trump and most US governors imposed heavy restrictions on people’s freedom. The purpose, said Trump and his COVID-19 advisers, was to “flatten the curve”: shut down people’s mobility for two weeks so that hospitals could catch up with the expected demand from COVID patients. In her book Silent Invasion, Dr. Deborah Birx, the coordinator of the White House Coronavirus Task Force, admitted that she was scrambling during those two weeks to come up with a reason to extend the lockdowns for much longer. As she put it, “I didn’t have the numbers in front of me yet to make the case for extending it longer, but I had two weeks to get them.” In short, she chose the goal and then tried to find the data to justify the goal. This, by the way, was from someone who, along with her task force colleague Dr. Anthony Fauci, kept talking about the importance of the scientific method. By the end of April 2020, the term “flatten the curve” had all but disappeared from public discussion.
Now that we are four years past that awful time, it makes sense to look back and see whether those heavy restrictions on the lives of people of all ages made sense. I’ll save you the suspense. They didn’t. The damage to the economy was huge. Remember that “the economy” is not a term used to describe a big machine; it’s a shorthand for the trillions of interactions among hundreds of millions of people. The lockdowns and the subsequent federal spending ballooned the budget deficit and consequent federal debt. The effect on children’s learning, not just in school but outside of school, was huge. These effects will be with us for a long time. It’s not as if there wasn’t another way to go. The people who came up with the idea of lockdowns did so on the basis of abstract models that had not been tested. They ignored a model of human behavior, which I’ll call Hayekian, that is tested every day.
These are the opening two paragraphs of my latest Defining Ideas article, “Looking Back at COVID’s Authoritarian Regimes,” Defining Ideas, March 14, 2024.
Another excerpt:
That wasn’t the only uncertainty. My daughter Karen lived in San Francisco and made her living teaching Pilates. San Francisco mayor London Breed shut down all the gyms, and so there went my daughter’s business. (The good news was that she quickly got online and shifted many of her clients to virtual Pilates. But that’s another story.) We tried to see her every six weeks or so, whether that meant our driving up to San Fran or her driving down to Monterey. But were we allowed to drive to see her? In that first month and a half, we simply didn’t know.
Read the whole thing, which is longer than usual.
(0 COMMENTS) budget deficit coronavirus covid-19 white house fauci trump canada

Problems After COVID-19 Vaccination More Prevalent Among Naturally Immune: Study


For-profit nursing homes are cutting corners on safety and draining resources with financial shenanigans − especially at midsize chains that dodge public scrutiny


‘Excess Mortality Skyrocketed’: Tucker Carlson and Dr. Pierre Kory Unpack ‘Criminal’ COVID Response


Looking Back At COVID’s Authoritarian Regimes


Trump nearly derailed democracy once − here’s what to watch out for in reelection campaign


Health Officials: Man Dies From Bubonic Plague In New Mexico


Stock Market Today: Stocks turn lower as factory inflation spikes, retail sales miss target


The SNF Institute for Global Infectious Disease Research announces new advisory board


Five Aerospace Investments to Buy as Wars Worsen Copy


COVID-19 vaccines: CDC says people ages 65 and up should get a shot this spring – a geriatrician explains why it’s vitally important
-

 Uncategorized3 weeks ago
Uncategorized3 weeks agoAll Of The Elements Are In Place For An Economic Crisis Of Staggering Proportions
-

 International1 week ago
International1 week agoEyePoint poaches medical chief from Apellis; Sandoz CFO, longtime BioNTech exec to retire
-

 Uncategorized4 weeks ago
Uncategorized4 weeks agoCalifornia Counties Could Be Forced To Pay $300 Million To Cover COVID-Era Program
-

 Uncategorized3 weeks ago
Uncategorized3 weeks agoApparel Retailer Express Moving Toward Bankruptcy
-

 Uncategorized4 weeks ago
Uncategorized4 weeks agoIndustrial Production Decreased 0.1% in January
-

 International7 days ago
International7 days agoWalmart launches clever answer to Target’s new membership program
-

 Spread & Containment2 days ago
Spread & Containment2 days agoIFM’s Hat Trick and Reflections On Option-To-Buy M&A
-

 Uncategorized4 weeks ago
Uncategorized4 weeks agoRFK Jr: The Wuhan Cover-Up & The Rise Of The Biowarfare-Industrial Complex